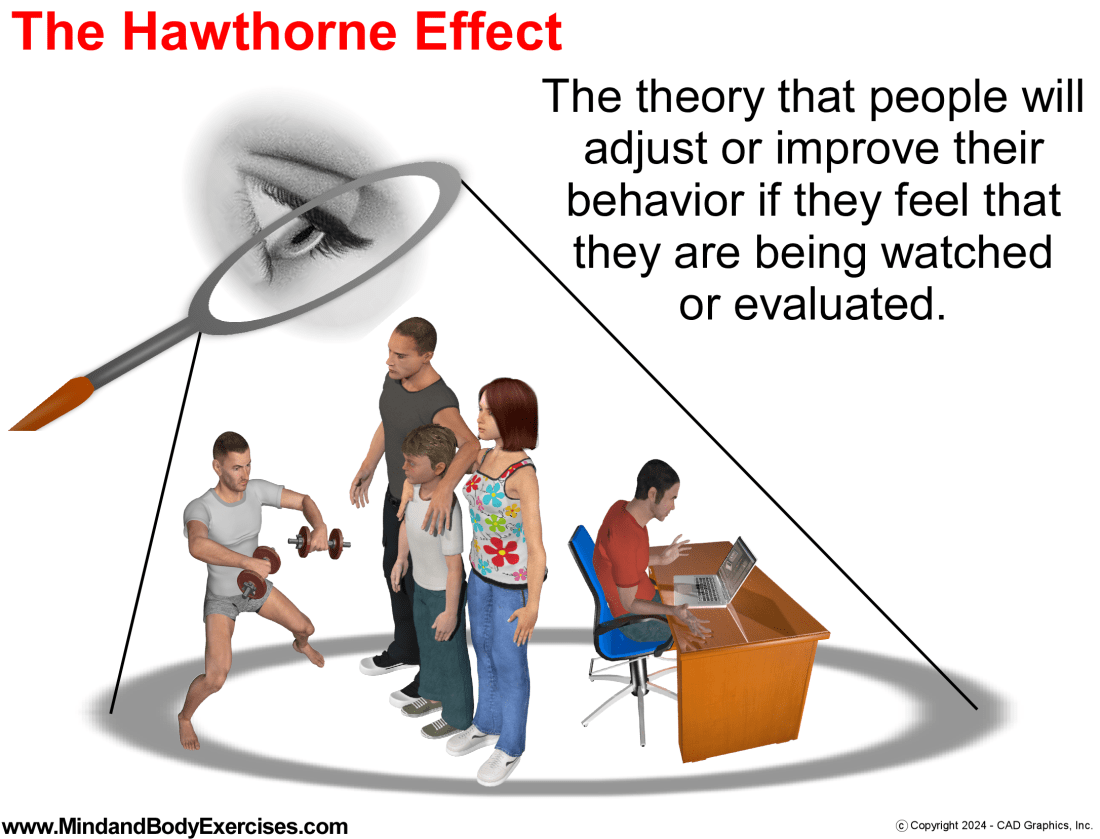
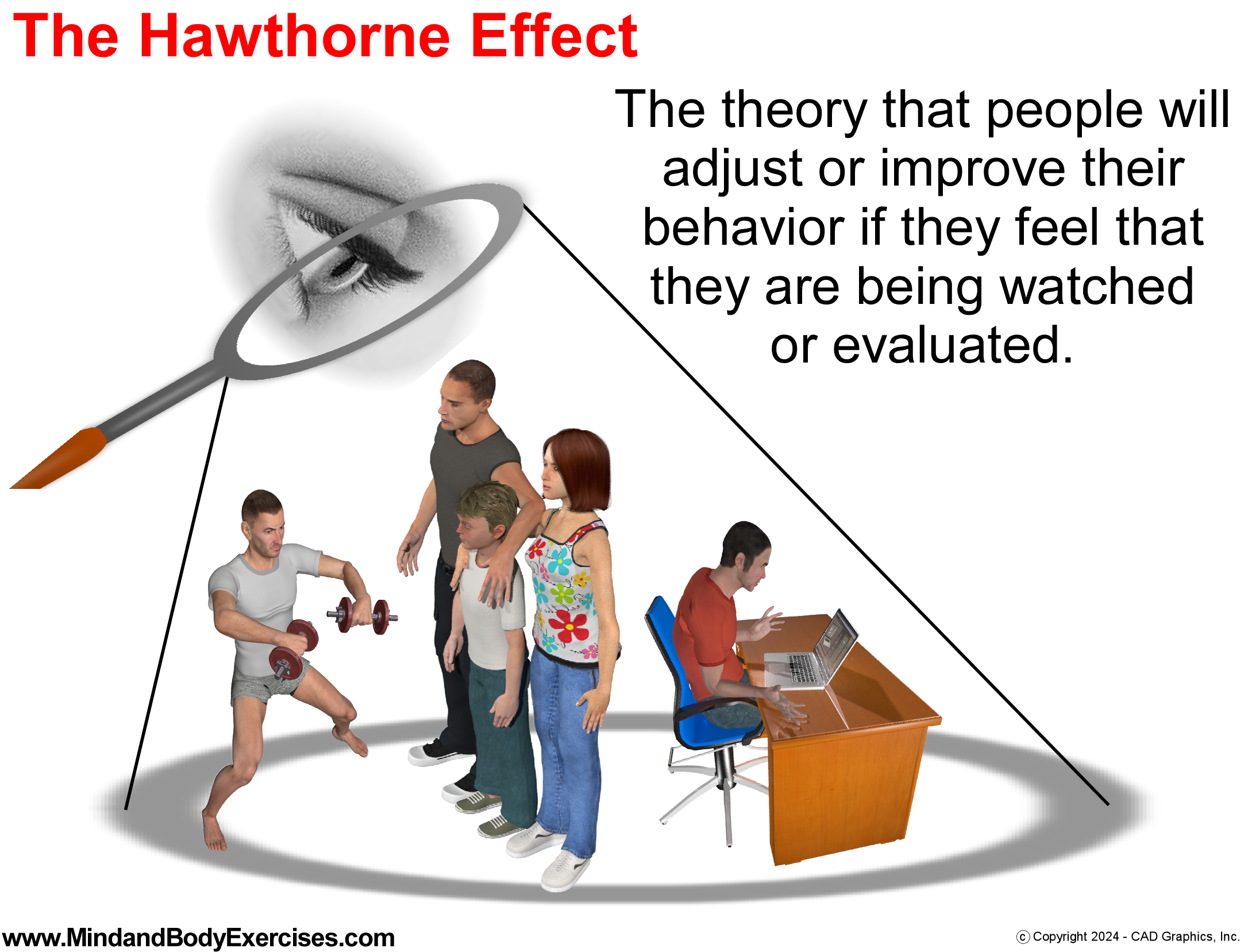
The Hawthorne Effect in Modern Contexts: Workplace, Gym, and Family Dynamics
The Hawthorne Effect refers to the tendency for individuals to alter their behavior when they are aware they are being observed. This aspect of human behavior was discovered during the Hawthorne Studies conducted at the Western Electric Company in Chicago, Illinois during the 1920s. This effect highlights how observation can influence performance and attitudes (McCambridge et al., 2014). In today’s interconnected and highly surveillance society, this phenomenon has notable implications for various environments, ranging not only in the workplace, but at the gym, in social settings, and even within family settings in public.
I can relate this back to my personal experiences while training in martial arts as a young adult. My teachers would often drive the point home that it was important and recognized when students worked hard and diligently while at the school in the group training environment. However, it was even more important how we trained on our own individually when no one else was around us or watching our work ethic in the solo setting. Similarly, the famous psychologist Carl Jung proposed the concept of each of us having our “shadow” or the hidden aspects of our behavior that we don’t usually show in public. When we know we are being observed the shadow part of one’s character hides and in place, various “personas” step up to match the situation and relative environment. In some settings, this may be perceived by others as “putting on an act,” or being a hypocrite.
Workplace Applications of the Hawthorne Effect
The Hawthorne Effect remains highly relevant to today’s workplace environment, especially as business organizations emphasize performance management and workplace culture. When employees are aware that their supervisors or peers are watching, they are more likely to engage in positive behaviors, such as increasing productivity and adhering to company protocols and policies. Studies have shown that the awareness of being observed can nurture a temporary boost in motivation and morale (Sedgwick & Greenwood, 2015). However, too heavily relying on this effect for performance enhancement may lead to superficial compliance rather than sustained engagement, consequently masking underlying workplace issues that affect productivity (McCambridge et al., 2014).
The Hawthorne Effect at the Gym
The Hawthorne Effect is also prevalent in fitness settings. Individuals at the gym, yoga studio or other fitness venues often push themselves harder or adopt better form when they believe others are observing them. This phenomenon is especially evident in both group exercise classes and during personal training sessions. The effect of observation may enhance short-term effort, but it can also create unrealistic standards of performance and an environment of comparison. Research suggests that social comparison in gym settings can both motivate and hinder progress, depending on the individual’s self-perception and fitness goals (Diel et al., 2021).
Family Dynamics in Public Spaces
The Hawthorne Effect extends to family dynamics in public as well, where the presence of other people can influence how family members interact with each other. Parents may become more patient or attentive to their children, and couples may show more affection. This effect speaks to the human tendency to present an idealized version of oneself in front of others, often reflecting societal expectations (Sedgwick & Greenwood, 2015). Although the intent may be positive, consistently modifying behavior based on external perceptions can hinder authentic interactions and create strain within relationships, as it sets up expectations that may not align with everyday family dynamics.
Conclusion
This phenomenon of human behavior demonstrates how the awareness of observation can influence temporary changes in behavior across various settings. While it can serve as a motivator in the workplace and gym, or encourage positive family or social network interactions in public, over-reliance on this effect may lead to superficial or unsustainable behavior changes. Realizing the implications of the Hawthorne Effect can encourage more genuine engagement and support environments that encourage authenticity over performative behaviors.
References
Diel, K., Broeker, L., Raab, M., & Hofmann, W. (2021). Motivational and emotional effects of social comparison in sports. Psychology of Sport and Exercise, 57, 102048. https://doi.org/10.1016/j.psychsport.2021.102048
McCambridge, J., Witton, J., & Elbourne, D. R. (2013). Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. Journal of Clinical Epidemiology, 67(3), 267–277. https://doi.org/10.1016/j.jclinepi.2013.08.015
I teach and offer lectures about holistic health, physical fitness, stress management, human behavior, meditation, phytotherapy (herbs), music for healing, self-massage (acupressure), Daoyin (yoga), qigong, tai chi, and baguazhang.
Please contact me if you, your business, organization, or group might be interested in hosting me to speak on a wide range of topics related to better health, fitness, and well-being.
I look forward to further sharing my message by partnering with hospitals, wellness centers, VA centers, schools on all levels, businesses, and individuals who see the value in building a stronger nation through a healthier population.
I also have hundreds of FREE education video classes, lectures, and seminars available on my YouTube channel at:
The Hero’s Journey outline can apply to the average person’s life by representing the various stages of growth and transformation that almost everyone experiences. In our own personal journeys, we may all experience different circumstances or perceptions. There is only one truth, but infinite perceptions for any particular event. In real life, this journey could look like facing major life changes, pursuing personal goals, or overcoming significant mental, physical, and even spiritual challenges.
Here’s how it might play out in the life of an everyday person:
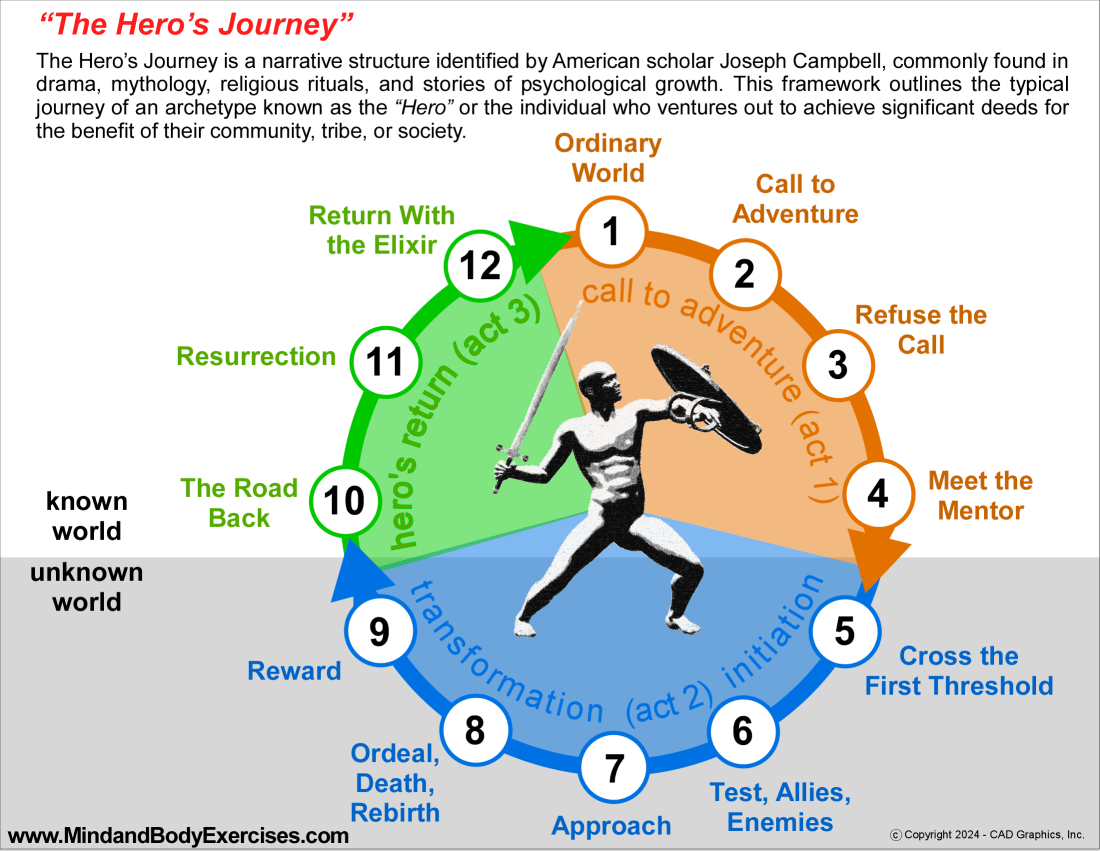
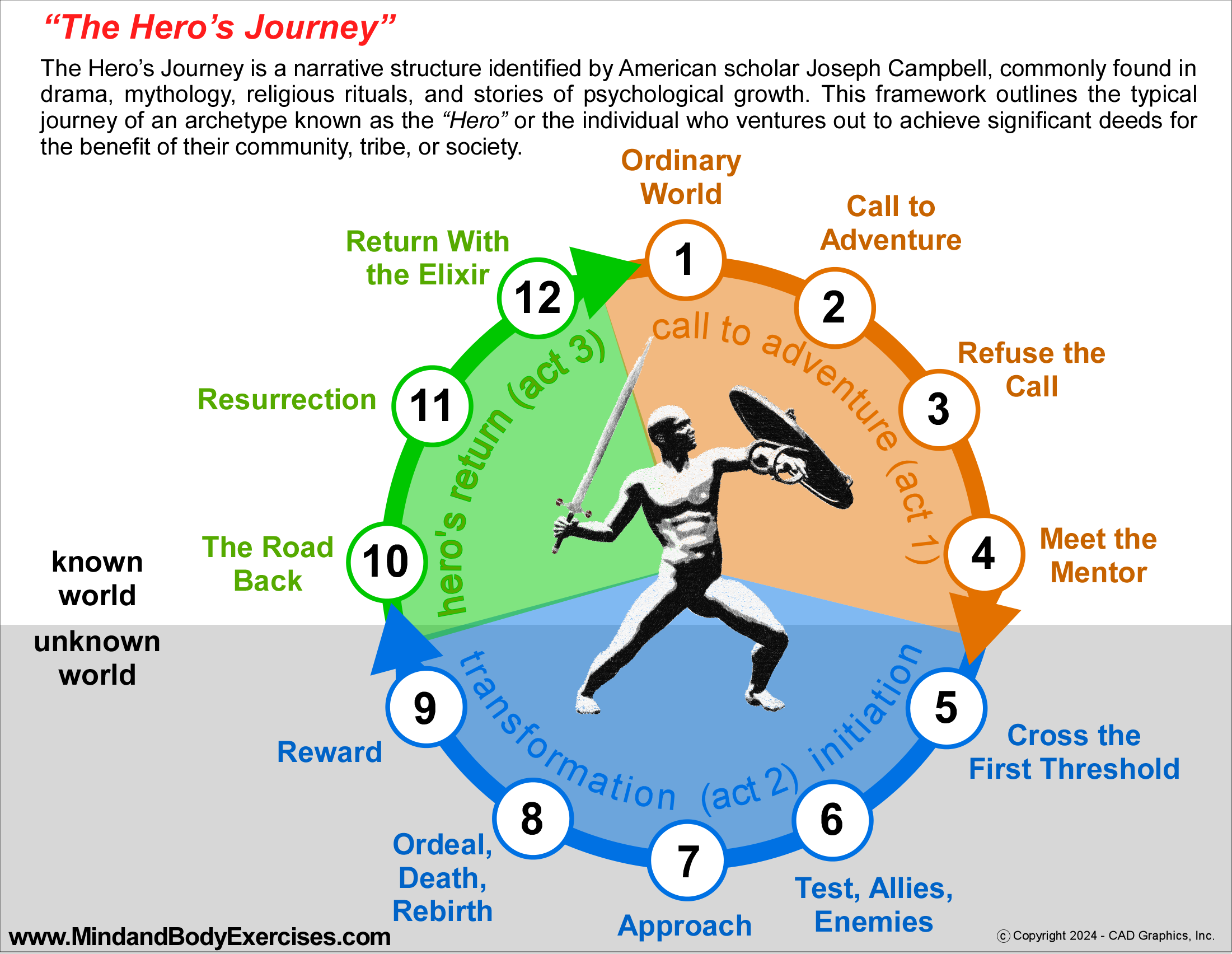
The steps of the “Hero’s Journey” include:
1- THE ORDINARY WORLD: The hero is often unaware, uneasy, or facing internal conflict, is introduced in a relatable way, allowing the audience to connect with their personal situation or struggle. The hero’s background of environment, family, and personal history, is established, revealing a feeling of opposing forces that pull the hero in different directions, creating mental and physical tension. (REAL WORLD APPLICATION: We might feel dissatisfied or unsure about something but aren’t yet driven to make a change)
2 – THE CALL TO ADVENTURE: A change is introduced to the not-yet hero, either through external forces or an internal realization, which compels the hero to confront an initial shift in their life. Something happens that urges us to change—a new job offer, a health issue, a relationship shift, or simply a sense of restlessness pushing us to grow. (REAL WORLD APPLICATION: Something happens that urges us to change such as a new job offer, a health issue, a relationship shift, or simply a sense of restlessness pushing us to grow.)
3 – REFUSAL OF THE CALL: The hero initially resists the journey, feeling uncertainty, fear of the unknown or a desire to turn away. In some cases, another 3rd party character may voice these fears and the risks involved. (REAL WORLD APPLICATION:Most often, our first reaction is resistance. We might feel afraid, overwhelmed, or doubt if we’re capable of taking on the new challenge.)
4 – MEETING WITH THE MENTOR: The hero encounters an experienced guide who provides knowledge, wisdom, training, resources, or crucial advice for the journey ahead. The hero is forced or accepts to look inward to find courage and inner wisdom. (REAL WORLD APPLICATION: In real life, mentors come in many forms like family members, friends, a teacher, a therapist, or even an inspiring book or experience that gives us insight or guidance.)
5 – CROSSING THE THRESHOLD: At the end of the first act, the hero commits to leaving behind the “ordinary world” and stepping into a new realm, filled with unknown rules and values. (REAL WORLD APPLICATION: This is the moment we commit to the journey, stepping out of our comfort zone. It could be moving to somewhere else, leaving a job, or simply deciding to make a big life change.)
6 – TESTS, ALLIES, AND ENEMIES: The hero faces various challenges, cultivates alliances, and identifies challenges and adversaries in the new world. (REAL WORLD APPLICATION: On our journey forward, we may encounter challenges and discover who supports or hinders us. We might face setbacks, doubts or obstacles while finding allies who encourage us.)
7 – APPROACH: With newly forged alliances, the hero prepares for a major trial or challenge within this unfamiliar world. (REAL WORLD APPLICATION:As we get closer to our goal, we prepare for a major challenge. This could mean making a big presentation, taking a final exam, or confronting an important fear.)
8 – THE ORDEAL: Near the story’s midpoint, the hero reaches a pivotal moment in the “unknown world,” confronting injury, death or their deepest fear. This moment of confrontation brings about a form of transformation, rebirth or renewal. (REAL WORLD APPLICATION:This is the peak moment where we face a major hurdle, fear or obstacle, like overcoming a health crisis, finally letting go of a limiting belief, or facing a major confrontation. It feels like a personal “death and rebirth,” as we emerge stronger and changed.)
9 – THE REWARD: The hero claims the reward or treasure that results from facing their challenges. There may be a celebration, though there is often still a risk of losing the reward. (REAL WORLD APPLICATION: Having faced our ordeal, we gain something valuable like greater confidence, resilience, insight, or a concrete achievement that represents our growth.)
10 – THE ROAD BACK: Around two-thirds into the story, the hero is driven to finish the adventure, returning from the unknown world to ensure the reward makes it home. Sometimes a chase scene highlights the mission’s urgency and very possibly danger. (REAL WORLD APPLICATION:With new insight or skills, we may be driven to bring our growth back to our everyday lives, sometimes facing new challenges as we try to integrate our journey’s rewards.)
11 – THE RESURRECTION: At the story’s climax, the hero undergoes a final, intense test as they approach home. They are transformed by a last act of defying death, embracing rebirth, or a sacrifice of some major merit, reaching a higher state of completion. Through the hero’s actions, the initial conflicts find resolution. (REAL WORLD APPLICATION: Before fully returning to our “normal” life, we’re often tested again, reinforcing our inner transformation. This could mean facing a problem like the one we just faced before but responding differently due to our growth.)
12 – RETURN WITH THE ELIXIR: The hero returns or continues the journey, now possessing a reward, treasure (or elixir) with transformative power, both for the hero and for the world they return to. (REAL WORLD APPLICATION: Finally, we bring valuable aspects to our daily life, whether it’s wisdom, resilience, or a new perspective. Our journey may not only transform us, but often positively impacts those around us.)
In our real life, these stages might be less dramatic and more cohesive, and maybe even more blended together. The Hero’s Journey reminds us that life is a series of growth cycles, and each challenge we face can lead to transformation, making us more resilient, self-aware, and capable.
The Perception of Healthy Eating as a Privilege in the U.S. Healthcare Landscape
Today in the US, access to nutritious food is often perceived as a privilege rather than a basic necessity. There is a combination of systemic issues in the food and healthcare industries, social inequality, and perhaps a narrow public understanding of just what good health consists of. These issues have contributed to driving up the cost of nutritious food, creating significant obstacles to maintaining a healthy balanced diet. Ironically, as US healthcare costs continue to rise dramatically, the consumption of unhealthy foods contributes to chronic health conditions creating a vicious circle of events that push individuals further into the healthcare system and consequently perpetuating the cycle of preventable diseases. These are factors that in the US, have shaped the perception that eating healthfully is a luxury and how this perception stems from economic, cultural, and educational factors that influence food choices, physical health, and overall well-being.
Economic Constraints: Why Healthy Food Costs More
A simple reason for the perception of healthy eating as a luxury is the cost disparity between purchasing of nutritious and non-nutritious foods. Organic, fresh, and minimally processed foods are typically more expensive due to significant factors such as agricultural practices, supply chain logistics, and governmental subsidies (Ver Ploeg et al., 2015). Organic farming methods are more labor-intensive and produce lower crop yields compared to of conventional farming, which relies more heavily on use of chemical pesticides and fertilizers (Hughner et al., 2007). This added labor cost, along with a limited supply, increases the cost of organic food, making it less accessible to individuals with lower incomes (Ver Ploeg et al., 2015). Conversely, crops like soy, corn, and wheat, which are often genetically modified and treated with chemicals, are heavily subsidized by the U.S. government, making processed foods derived from these crops less expensive for consumers. This economic landscape perpetuates a cycle where affordable, nutritionally poor food is more accessible, while healthier options remain financially out of reach.
Processed Foods: The Price of Convenience
Aside from cost, processed foods that are loaded with sweeteners, artificial preservatives, and flavor enhancers are designed for maximum taste appeal, convenience, and shelf stability. These foods are quite often high in sugars, salt, and unhealthy fats, all of which contribute to obesity, diabetes, and cardiovascular disease (Monteiro et al., 2018). Low-income neighborhoods, where grocery stores lack fresh produce, frequently rely on this calorie-dense but nutritionally lacking products. The convenience and affordability of these foods cloud the fact that they are contributors to poor health when consumed long-term. The perception that eating healthy is a privilege, reflects not only the cost of food but also the accessibility and desire for unhealthful options that fit into the American fast-paced, budget-conscious lifestyles (Ver Ploeg et al., 2015).
Education and Health Literacy: The Hidden Barrier
A major factor adding to this issue is a lack of health education and literacy among the general population. Understanding the impact of nutrition on long-term health is not prioritized in many US schools, and misinformation about what constitutes “healthy” is extensive (Nestle, 2013). Marketing campaigns often mislead consumers into thinking that “sugar-free” or “low-fat” foods are healthy. In reality, these foods often contain harmful additives like high-fructose corn syrup or aspartame, which both have been linked to various health risks (Swithers, 2015). Also, public knowledge of the role of whole foods, hydration, and balanced macronutrient intake is often dismal, leading some to make choices that encourage immediate taste satisfaction over long-term health benefits (Nestle, 2013). As a result, the cultural perception of healthful food as a luxury is partly fueled by a lack of nutritional knowledge, leading individuals to turn to less expensive, popular foods over healthier, less well-understood options.
The Institutional Influence: Schools and Healthcare
Schools and the healthcare system also shape public perception and access to healthy food. School meal programs, specifically those in lower-income areas, often offer highly processed foods due to budget constraints and limited resources for fresh ingredients (Gaines et al., 2014). This reinforces the idea that nutrient-dense foods are exceptional rather than essential. Just as the U.S. healthcare system prioritizes treatment over prevention, schools rarely encourage dietary education as part of comprehensive healthcare (Schroeder, 2007). While medical professionals widely recognize the link between diet and chronic disease, the system rarely encourages preventive approaches, including education relative to nutrition and lifestyle changes (Schroeder, 2007). This gap leaves many young Americans, especially those without access to nutritional education, without a clear understanding of how a healthy diet influences long-term health.
Bottled Water vs. Sugary Beverages: A Reflection of Misplaced Priorities
The fact that bottled water costs more than soda and soft drinks reflects the prioritization of profit over public health. Soda and other sugary beverages are relatively cheap due to subsidies for their ingredients and widespread production. Bottled water prices remain high due to packaging and branding processes. This pricing paradox encourages consumers, particularly those with limited resources to choose soda over water. The strategic marketing of sugary drinks as less-expensive alternatives further contributes to poor dietary habits and supports the idea that basic, healthy choices are a privilege for the exclusive or elitist.
Breaking the Cycle: A Call for Systemic Change
Recognizing and addressing the perception of having a healthy diet, being a privilege requires systemic changes across multiple sectors. Lawmakers must evaluate agricultural subsidies to level the playing field between nutrient-dense foods and heavily processed products (Miller et al., 2016). Schools should encourage nutritional education and pursue methods to improve food quality within budgetary limits, especially in low-income areas (Gaines et al., 2014). Additionally, healthcare providers should encourage preventive care practices that focus on dietary education, empowering patients to make more informed food choices. With these changes, healthy eating can become more accessible and implemented.
In conclusion, the view of healthy eating as a luxury reflects societal inequities within the American food and healthcare systems. By reducing economic and informational barriers to nutritious food, American society can cultivate a culture where healthy choices are more available to everyone, making better health and well-being, not a privilege but a shared right.
References
Gaines, A. B., Lonis-Shumate, S. R., & Gropper, S. S. (2011). Evaluation of Alabama public school wellness policies and state school mandates. Journal of School Health, 81(5), 281-287. https://doi.org/10.1111/j.1746-1561.2011.00588.x
Hughner, R. S., McDonagh, P., Prothero, A., Shultz, C. J., & Stanton, J. (2007). Who are organic food consumers? A compilation and review of why people purchase organic food. Journal of Consumer Behaviour, 6(2-3), 94-110. https://doi.org/10.1002/cb.210
Monteiro, C. A., Cannon, G., Levy, R. B., Moubarac, J.-C., Jaime, P., Martins, A. P., … & Swinburn, B. (2018). Ultra-processed foods: What they are and how to identify them. Public Health Nutrition, 21(1), 6-8. https://doi.org/10.1017/S1368980018003762
Schroeder, S. A. (2007). We can do better—improving the health of the American people. New England Journal of Medicine, 357(12), 1221-1228. https://doi.org/10.1056/NEJMsa073350
Ver Ploeg, M., Mancino, L., Todd, J. E., Clay, D. M., & Scharadin, B. (2015). Where do Americans usually shop for food and how do they travel to get there? Initial findings from the National Household Food Acquisition and Purchase Survey. U.S. Department of Agriculture, Economic Research Service.
I teach and offer lectures about holistic health, physical fitness, stress management, human behavior, meditation, phytotherapy (herbs), music for healing, self-massage (acupressure), Daoyin (yoga), qigong, tai chi, and baguazhang.
Please contact me if you, your business, organization, or group might be interested in hosting me to speak on a wide range of topics related to better health, fitness, and well-being.
I look forward to further sharing my message by partnering with hospitals, wellness centers, VA centers, schools on all levels, businesses, and individuals who see the value in building a stronger nation through a healthier population.
I also have hundreds of FREE education video classes, lectures, and seminars available on my YouTube channel at:
The Medicalization of Health: From Lifestyle Adjustments to Pharmaceuticals
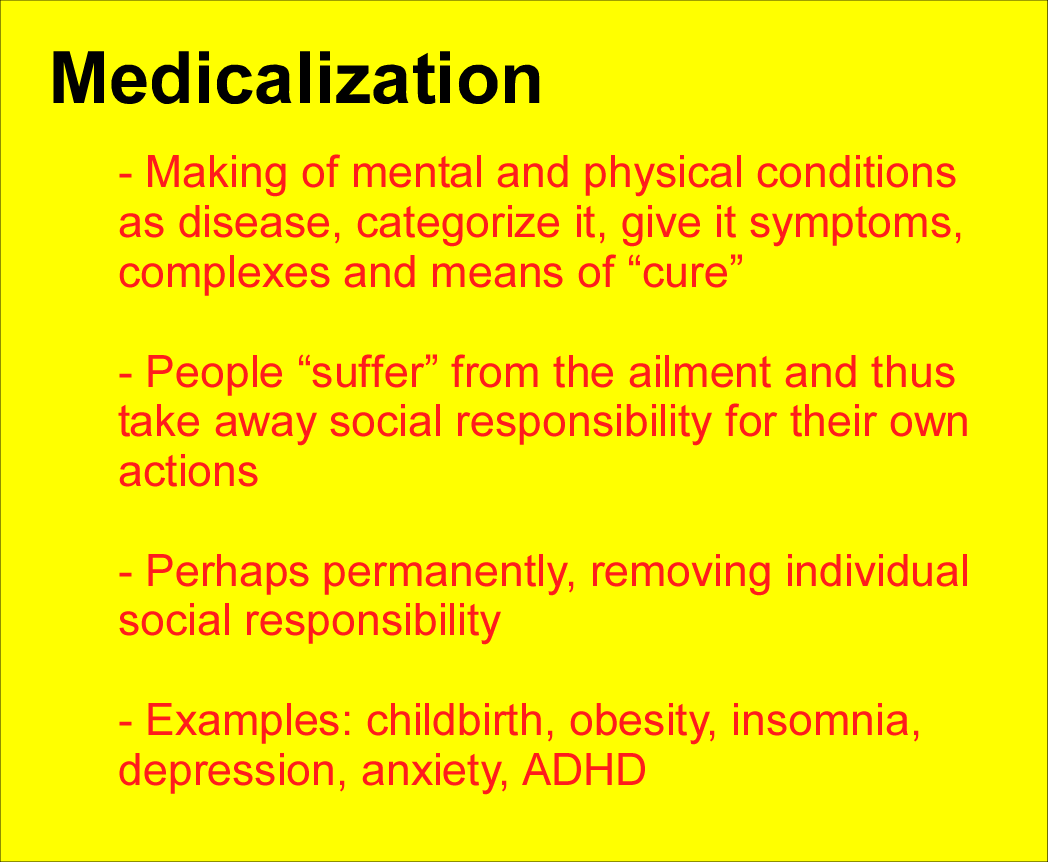
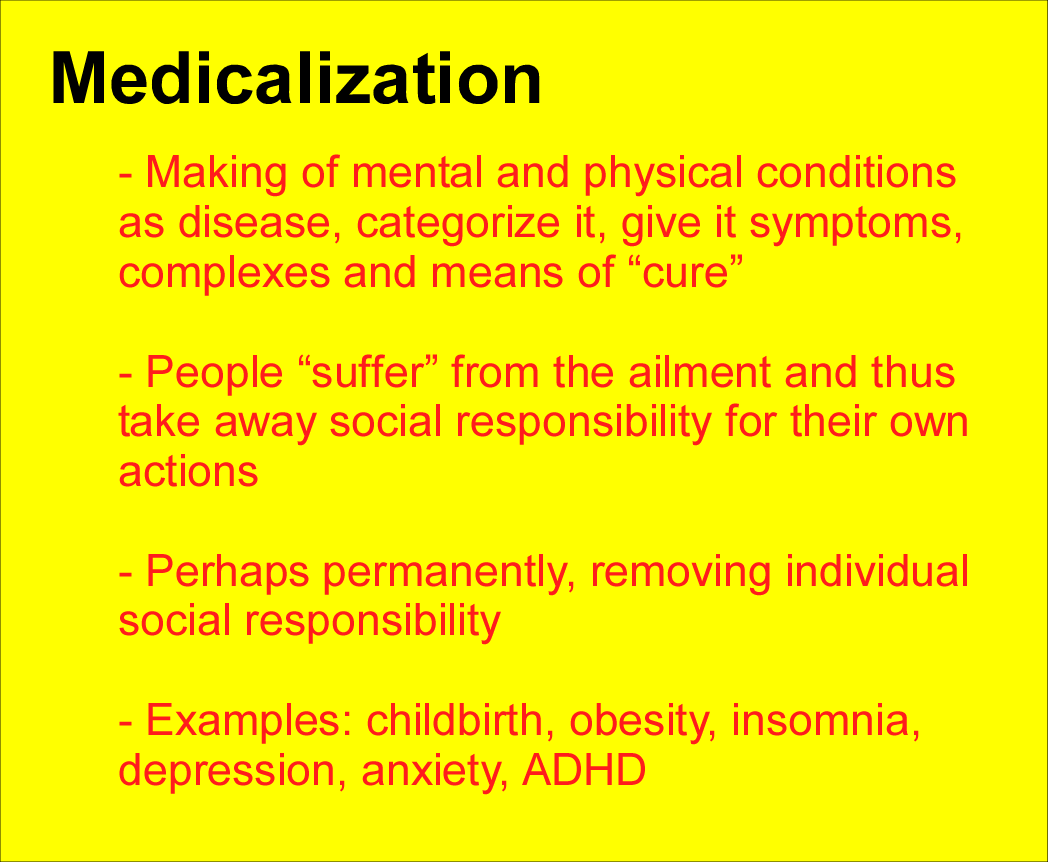
In recent decades, the US healthcare system has shifted toward addressing various health conditions through clinical interventions rather than lifestyle changes. This is now a trend referred to as “medicalization”. Medicalization involves labeling natural processes and/or lifestyle-related conditions as medical conditions that require pharmaceutical or surgical treatments as the preferred solutions. Health issues such as childbirth, obesity, depression, ADHD, anxiety, insomnia, and others, were once managed with diet, exercise, and social support. In years past these issues were seen as part of the human experience. These ailments are now frequently treated with drugs or invasive procedures. Medicalization offers rapid solutions but also raises concerns about the rise in pharmaceutical dependence and how consumer influence is encouraging this shift.
Suppose Western allopathic medicine and medicalizing conditions are considered safe and effective treatments. Why are we seeing all-time highs in these areas?
Infant Mortality: The U.S. infant mortality rate rose to 5.6 deaths per 1,000 live births in 2022, marking the first increase in two decades, up by approximately 3% from 2021. This trend varies across racial and ethnic groups, with significant increases noted among infants of American Indian and Alaska Native mothers CDC CDC Blogs.
Obesity: Among U.S. adults, obesity prevalence was last recorded at 41.9% by the CDC. This figure has seen a steady increase over the years and reflects long-term trends rather than recent spikes.
Depression: The National Institute of Mental Health (NIMH) reports that 8.4% of U.S. adults experienced at least one major depressive episode in 2022. This aligns closely with your figure and indicates an increase in mental health issues, especially post-pandemic.
ADHD: For children ages 3–17, ADHD prevalence remains close to 10%, with recent surveys indicating about 9.8% are diagnosed with ADHD. Your figure of 11.4% is slightly higher than the current average but within a plausible range, considering increases in diagnosis rates over the past few years.
Anxiety: Anxiety disorders affect around 31% of U.S. adults at some point, according to the NIMH. This remains one of the most common mental health conditions, with prevalence rising, particularly among younger adults.
Insomnia: Roughly 14.5% of adults report experiencing chronic sleep issues, including difficulty falling asleep most nights, a condition that is increasingly recognized as widespread in the U.S. population.
Treating symptoms without addressing the root causes of disease and illness, creates pharmaceutical customers for the long term, without effectively curing anything.
Direct-to-Consumer Pharmaceutical Advertising in the U.S. and New Zealand
The United States and New Zealand are the only countries allowing direct-to-consumer (DTC) pharmaceutical advertising, fueling the perception that medication is the primary route to wellness. With advertisements that are seen on television, in print, and online, drugs are marketed as quick and simple solutions to complex health issues, often emphasizing benefits while dismissing potential risks (Ventola, 2011). Such advertising encourages a culture where consumers may feel the need or desire for medications for issues that may otherwise be managed without drugs. This situation consequently drives demand for pharmaceutical solutions and potentially contributes to overdiagnosis and overtreatment (Ventola, 2011).
Role of Medical Professionals and Consumer Complacency
Medical professionals play a major part in driving medicalization. Pressured by patient demand for immediate solutions and limited consultation time, physicians may prioritize pharmaceutical treatments over lifestyle-based recommendations (Topol, 2015). Pharmaceutical companies knowingly promote their products to healthcare providers, offering the immediate solutions that medications may offer compared to lifestyle changes. Consumer demand favors this approach, where patients seek medications for conditions that could potentially be addressed through diet, exercise, or mental health practices (Moynihan et al., 2002). This dependency on pharmaceuticals creates a cycle of reliance, diminishing the desire for individuals to manage their own health through more sustainable means.
Medicalization of Childbirth
Throughout much of human history, childbirth was a natural process, often managed by midwives and family members (Simonds et al., 2007). Childbirth, especially in the US, has become highly medicalized, with many births taking place in hospitals with the usage of epidurals, Cesarean sections, and labor-inducing drugs. In the United States, the Cesarean section rate is nearly 32%, exceeding World Health Organization (WHO) recommendations of 10–15% (WHO, 2015). The routine use of medical interventions in low-risk pregnancies has led to concerns about unnecessary risks and a sense of reduced autonomy among women (MacDorman et al., 2016). These interventions may help to ensure safety in high-risk situations, but critics argue that their frequent overuse may add stress, complications, and an overemphasis on medical control (Simonds et al., 2007).
Obesity: The Turn to Medications and Surgery
Obesity is now seen as a medical condition, despite it being greatly influenced by lifestyle factors such as diet and exercise. Medications as well as surgeries, such as gastric bypass, have become common solutions despite the WHO’s emphasis on lifestyle interventions as first-line responses (WHO, 2021). Pharmaceutical options may provide rapid results and meet consumer demand for quick fixes. However, they often fail to tackle underlying factors like mental health, socioeconomic status, and environmental issues (Gaesser et al., 2021). The medicalization of obesity also reflects societal expectations for quick results, where lifestyle-based treatments are often seen as secondary (Gaesser et al., 2021).
Depression and Pharmaceutical Solutions
Depression was once regarded as a deeply personal struggle, has now been typically treated through antidepressants, making them one of the most prescribed medications in the world (McManus et al., 2016). Antidepressants provide critical support for those with severe depression, while the use of these pharmaceuticals can obscure the benefits of non-drug interventions, such as therapy, exercise, and lifestyle adjustments (Cuijpers et al., 2021). Medical experts typically advocate for a combined approach, but the demand for rapid relief often drives consumers toward pharmaceuticals as the primary solution. This trend highlights concerns about potential long-term dependency and other risks of addressing symptoms without fully understanding underlying causes (Cuijpers et al., 2021).
The Rise of ADHD Diagnoses and Stimulant Use
Another mental ailment that has increased greatly in recent decades is ADHD. Stimulant medications have become the primary treatment (Visser et al., 2014). Medications that improve focus and relieve symptoms such as Ritalin and Adderall can also lead to dependency and behavioral side effects. Non-pharmaceutical interventions, such as behavioral therapy and parental training, are often underutilized, despite their effectiveness in managing ADHD (Molina et al., 2009). The great increase in ADHD diagnoses has led some researchers to question whether typical childhood behaviors are increasingly pathologized, leading to increased unnecessary use of medication (Visser et al., 2014).
Medicalization of Other Common Conditions
Other medical conditions reflect the trend toward medicalization such as:
Anxiety and Anti-Anxiety Medications: The increased prescription of anti-anxiety medications, such as benzodiazepines, often occurs without deeper inquiry into alternatives of several agents such as ashwagandha, passionflower, galphimia, echinacea, ginkgo, chamomile, lemon balm, valerian, and lavender, which can often manage symptoms without the potential risks of dependency (Garakani et al., 2020).
Sleep Disorders and Sleeping Pills: Insomnia is frequently treated with sleeping pills, even though non-drug approaches, such as sleep hygiene and lifestyle adjustments, often produce more sustainable results (Smith & Perlis, 2020).
Menopause and Hormone Replacement Therapy (HRT): Menopause is a natural process, where hormone replacement therapy (HRT) is frequently prescribed to address symptoms. While HRT can be beneficial, its risks and potential side effects bring light to the discussion for balanced approaches that implement lifestyle adjustments (Manson et al., 2016).
Conclusion
The medicalization of various health issues, ranging from childbirth to obesity, depression, anxiety, insomnia ADHD, and perhaps others, reflects a broader societal trend toward pharmaceutical dependency and reliance. Medical interventions are invaluable in many cases, however, the increased reliance on medications and clinical treatments for conditions historically managed through lifestyle adjustments raises many ethical and practical concerns. The influence of pharmaceutical companies and the current advertising permissiveness in the United States and New Zealand further highlight the much-needed balanced approach that encourages sustainable, lifestyle-based strategies along with clinical treatment options. Increased emphasis on non-pharmaceutical approaches can help empower individuals to take a more proactive role in their own health and cultivate more realistic long-term wellness.
References
Cuijpers, P., Stringaris, A., & Wolpert, M. (2020). Treatment outcomes for depression: challenges and opportunities. The Lancet Psychiatry, 7(11), 925–927. https://doi.org/10.1016/s2215-0366(20)30036-5
Gaesser, G. A., & Angadi, S. S. (2021). Obesity treatment: Weight loss versus increasing fitness and physical activity for reducing health risks. iScience, 24(10), 102995. https://doi.org/10.1016/j.isci.2021.102995
Garakani, A., Murrough, J. W., Freire, R. C., Thom, R. P., Larkin, K., Buono, F. D., & Iosifescu, D. V. (2020). Pharmacotherapy of Anxiety Disorders: Current and emerging treatment options. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.595584
MacDorman, M. F., Declercq, E., Cabral, H., & Morton, C. (2016). Recent increases in the U.S. maternal mortality rate: Disentangling trends from measurement issues. Obstetrics & Gynecology, 128(3), 447-455. https://doi.org/10.1097/AOG.0000000000001556
Manson, J. E., Chlebowski, R. T., Stefanick, M. L., Aragaki, A. K., Rossouw, J. E., Prentice, R. L., … & Anderson, G. (2013). Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA, 310(13), 1353-1368. https://doi.org/10.1001/jama.2013.278040
McManus, S., Bebbington, P., Jenkins, R., & Brugha, T. (2016). Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey 2014. A survey carried out for NHS Digital by NatCen Social Research and the Department of Health Sciences, University of Leicester-UCL Discovery. https://discovery.ucl.ac.uk/id/eprint/1518055/
Molina, B. S., Hinshaw, S. P., Swanson, J. M., Arnold, L. E., Vitiello, B., Jensen, P. S., … & MTA Cooperative Group. (2009). The MTA at 8 years: Prospective follow-up of children treated for combined-type ADHD in a multisite study. Journal of the American Academy of Child & Adolescent Psychiatry, 48(5), 484-500. https://doi.org/10.1097/CHI.0b013e31819c23d0
Moynihan, R., Heath, I., & Henry, D. (2002). Selling sickness: The pharmaceutical industry and disease mongering. BMJ, 324(7342), 886-891. https://doi.org/10.1136/bmj.324.7342.886
Simonds, W., & Rothman, B. K. (2007). Laboring on: Birth in transition in the United States. Routledge.
Perlis, M. L., Pigeon, W. R., Grandner, M. A., Bishop, T. M., Riemann, D., Ellis, J. G., Teel, J. R., & Posner, D. A. (2021). Why treat insomnia? Journal of Primary Care & Community Health, 12, 215013272110140. https://doi.org/10.1177/21501327211014084
Topol, E. J. (2015). The patient will see you now: The future of medicine is in your hands. Basic Books.
Ventola C. L. (2011). Direct-to-Consumer Pharmaceutical Advertising: Therapeutic or Toxic?. P & T : a peer-reviewed journal for formulary management, 36(10), 669–684.
Visser, S. N., Danielson, M. L., Bitsko, R. H., Perou, R., & Blumberg, S. J. (2014). Trends in the parent-report of health care provider-diagnosed and medicated ADHD: United States, 2003–2011. Journal of the American Academy of Child & Adolescent Psychiatry, 53(1), 34-46. https://doi.org/10.1016/j.jaac.2013.09.001
I teach and offer lectures about holistic health, physical fitness, stress management, human behavior, meditation, phytotherapy (herbs), music for healing, self-massage (acupressure), Daoyin (yoga), qigong, tai chi, and baguazhang.
Please contact me if you, your business, organization, or group might be interested in hosting me to speak on a wide range of topics related to better health, fitness, and well-being.
I look forward to further sharing my message by partnering with hospitals, wellness centers, VA centers, schools on all levels, businesses, and individuals who see the value in building a stronger nation through a healthier population.
I also have hundreds of FREE education video classes, lectures, and seminars available on my YouTube channel at: