Modern medicine is often imagined as a precise science, guided by objective data, advanced technologies, and well-established clinical procedures. Yet the reality, particularly in surgical practice, is far more complex, uncertain, and deeply human. Atul Gawande’s Complications: A Surgeon’s Notes on an Imperfect Science provides a candid exploration of this reality. Among its most revealing themes is the practice of Morbidity and Mortality (M&M) meetings, a long-standing tradition within hospitals that reflects medicine’s willingness to confront its own fallibility. These meetings are structured, routine gatherings where physicians review mistakes, unexpected complications, and patient deaths. They serve as one of the profession’s oldest and most honest mechanisms for learning, accountability, and institutional humility.

The Purpose and Structure of M&M Meetings
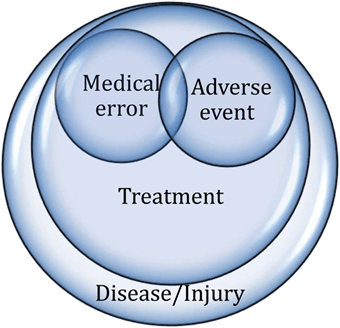
Every major surgical department holds M&M conferences at regular intervals, often weekly. These are not open to the public and typically include attending surgeons, residents, fellows, anesthesiologists, nurses, and other healthcare staff involved in patient care. A designated physician presents a recent case in which an adverse event occurred, such as an infection that spiraled out of control, a misdiagnosis that altered the course of treatment, a surgical decision that led to complications, or a death that was unexpected or preventable.
The goal is not punishment. Instead, the meeting operates on a principle of constructive scrutiny, where the presenter must outline what happened, why it happened, and how it could be prevented in the future. Other physicians then probe the case, raising questions or alternative approaches. Layers of clinical, ethical, and systemic variables are laid bare: Was the diagnosis delayed? Were symptoms misinterpreted? Did communication fail between team members? Did fatigue or inexperience contribute? Did systemic protocols fall short?
Within this setting, the case becomes a shared learning opportunity. For younger trainees, especially surgical residents, M&M offers some of the most memorable and sobering lessons of their careers. Gawande vividly describes how presenting at an M&M is both humbling and formative, forcing physicians to confront the tension between medicine’s ideals and its imperfect realities.

Fallibility and the Culture of Medicine
One of Gawande’s central insights is that medicine, despite its precision, is still a craft performed by human beings. Surgeons are trained through hands-on experience, meaning that early in their careers they inevitably make mistakes. M&M meetings embody this recognition. Rather than hiding errors, the profession institutionalizes their examination. In doing so, it reinforces a culture of humility, an acknowledgment that even seasoned surgeons cannot escape uncertainty, complexity, or human limitation.
This culture contrasts sharply with public expectations. Patients often imagine their physicians as infallible or at least near-perfect experts. Yet M&M reveals the opposite: physicians must make rapid decisions under pressure, interpret ambiguous symptoms, and rely on probability rather than certainty. By learning from one another in this setting, they refine their skills, sharpen their thinking, and internalize the ethical and emotional weight of their responsibility.
The Ethical and Emotional Landscape
Participating in an M&M is emotionally charged. For the presenting physician, it can be deeply uncomfortable to stand before colleagues and recount a mistake that harmed or may have harmed a patient. Feelings of guilt, shame, or self-doubt often surface, and Gawande notes how these emotions can shape a surgeon’s development. Yet the discomfort has a purpose: it anchors the ethical seriousness of the profession.
M&M meetings also engage difficult moral questions. What counts as preventable? When is a complication a matter of poor judgment versus unavoidable risk? How should responsibility be assigned in cases involving multiple team members? These questions rarely have simple answers, yet the discussion itself strengthens the collective moral awareness of the healthcare team.
Systemic Learning and Improvement
Beyond the individual, M&M meetings illuminate system failures, not just personal ones. Many medical mistakes arise from structural issues: unclear protocols, communication breakdowns, equipment problems, or workflow inefficiencies. By analyzing cases as a group, the institution can identify patterns that would otherwise remain hidden. This reflective process has contributed to widespread improvements in patient safety, protocol standardization, and quality-control initiatives over the past several decades.
In this way, M&M meetings function as a bridge between medicine’s scientific ambitions and its real-world practice. They transform personal experience into shared institutional knowledge, reinforcing the idea that error is not merely an individual flaw but a signal prompting system-wide change.
Medicine as an Imperfect Science
At the heart of Gawande’s argument is the idea that medicine will never be a perfectly predictable science. Human physiology varies, disease behaves unpredictably, and the clinician’s perspective is always limited. M&M meetings embrace this imperfection by acknowledging that complications are not anomalies; they are intrinsic to medical practice. The best physicians are not those who never err, but those who learn continuously, communicate transparently, and evolve with each challenge.
This recognition resonates far beyond the hospital. It reflects a broader truth about human skill, decision-making, and mastery: improvement requires honest confrontation with error, a willingness to reflect, and the humility to adjust course. Whether in medical training, martial arts disciplines, meditation, or intellectual study, the process of growth requires the courage to examine mistakes without denial.
A Model for Other Disciplines
One striking implication of the M&M model is its potential applicability to other fields. Many professions such as law enforcement, education, business, athletics, and others, operate under pressure and uncertainty, yet few embrace such formalized self-examination. Gawande suggests that medicine’s structured review of error offers a template: regular, honest, non-punitive reflection on failure can elevate performance and embed ethical awareness across any discipline.
Within my broader work on holistic development, martial arts philosophy, and mind-body training, the M&M concept aligns naturally with the ethos of self-cultivation: mastery arises from rigorously examining one’s actions, acknowledging missteps, and transforming experience into wisdom. Just as the warrior, scholar, and sage refine themselves through reflection, the surgeon refines technique, judgment, and character through the discipline of confronting complications.
Morbidity and Mortality meetings represent one of the most profound expressions of medicine’s humility. They expose the complexity of human error, the emotional and ethical burdens of clinical practice, and the necessity of continuous learning. By institutionalizing the examination of complications, the medical profession acknowledges its imperfection while striving toward greater competence, safety, and compassion. Gawande’s reflections reveal that behind the precision of surgery lies a culture shaped by self-scrutiny and the courage to face the uncomfortable truth that mastery is never complete. In embracing this truth, both medicine and the individuals who practice it become better equipped to serve, heal, and grow.
References:
Gawande, A. (2002). Complications: A surgeon’s notes on an imperfect science. Henry Holt & Co.
GeeksforGeeks. (2025, July 23). Difference between morbidity and mortality. GeeksforGeeks. https://www.geeksforgeeks.org/biology/difference-between-morbidity-and-mortality/








{kind=link}