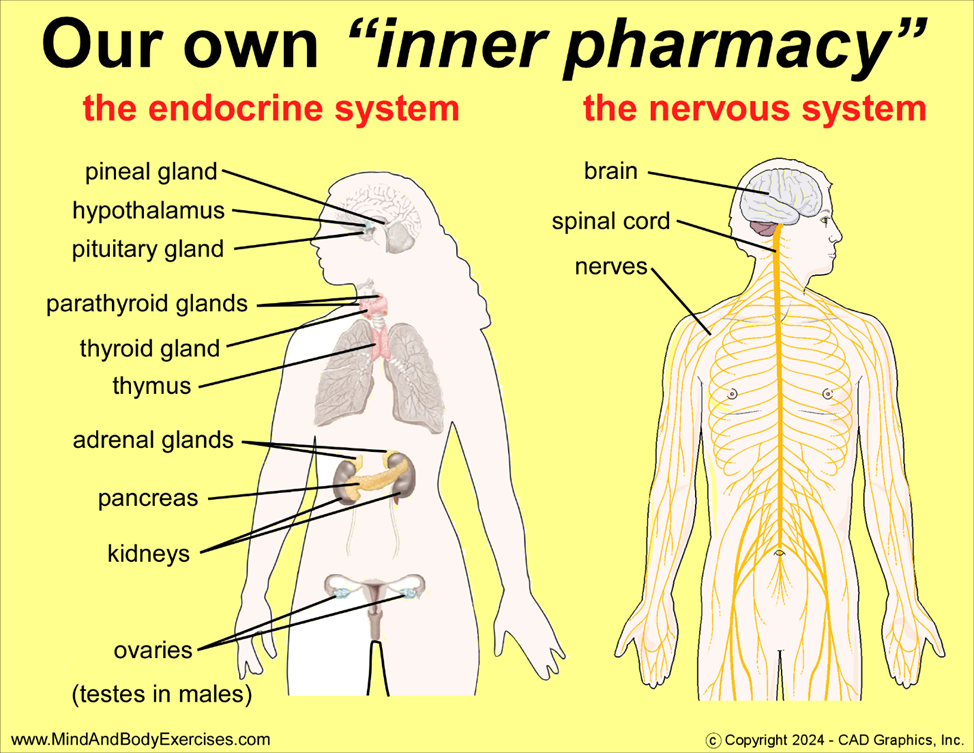
Energy Flow as Organ-to-Organ Transmission: Traditional Chinese Medicine (TCM) teaches that energy or “Qi” flows through the body in interconnected organ-to-organ patterns rather than simply circulating from the heart through the bloodstream. This insight reframes how we understand health and movement, emphasizing harmony and balance over mere exertion. This nuanced insight shifts the understanding of physical health from a single focal point to an interconnected system, encouraging movements designed to stimulate this flow comprehensively. This has profound implications for exercise design, rehabilitation, and even stress management, as it integrates bodily systems rather than isolating them.
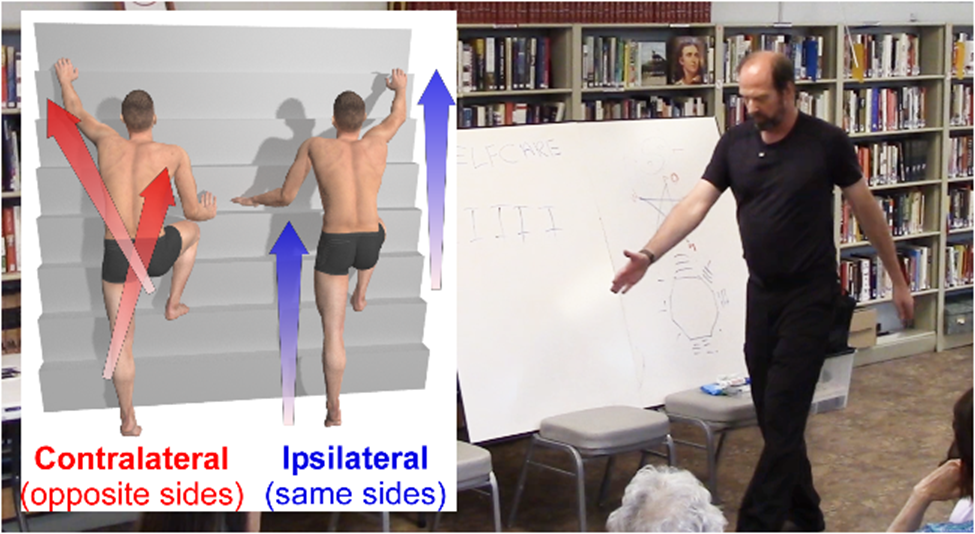
Asymmetry Designed for Functionality: Unlike common exercise patterns that often emphasize symmetrical movement for balance, the asymmetrical nature of these movements mimics biological energy pathways and ensures each part of the body receives appropriate stimulation and energy transfer. This ergonomic approach enhances efficiency and may reduce the chance of injury or overuse affecting one side more than the other.
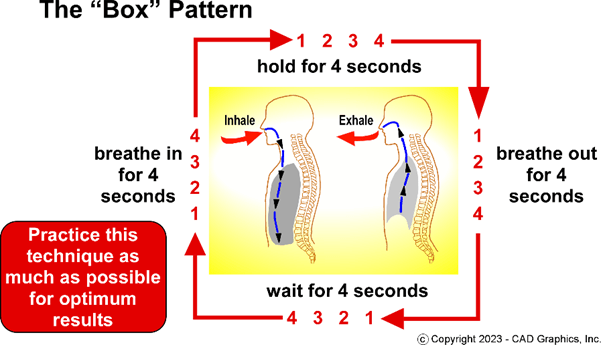
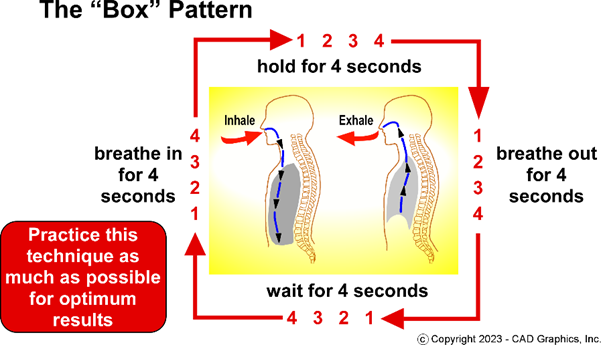
Breath Control and Relaxation Enable Deeper Energy Work: The synchronized breathing with physical movements, breathing in through the nose, out through the nose or mouth, and coordinating the tongue’s position, helps extend breath hold times, deepen relaxation, and conserve energy. The concept that tension reduces breath-holding capacity underscores the importance of mental calmness in physical performance and recovery, highlighting a mind-body connection often overlooked in Western fitness paradigms.
Joint Mobility and Energy Flow are Interlinked: The closing set’s focus on gently bending and releasing the major joints (shoulders, elbows, wrists, hips, knees, ankles) points to the joints as critical nodes for energy flow, not merely as mechanical hinges. This combined physical and energetic approach maintains joint flexibility and promotes a harmonious rhythm throughout the body, potentially preventing stiffness, spasms, and cramping after exercise.
Energy ‘Bank Account’ Metaphor Offers Sustainable Health Insight: By likening the body’s core energy center to a bank account, the practice teaches the value of replenishing energy rather than depleting it exclusively by movement. This metaphor aligns with modern concepts of energy management, self-care, and sustainability, emphasizing rest and recovery as essential for long-term health benefits, key for athletes, seniors, and anyone seeking balanced vitality.
Cultural Philosophy Enriches Physical Practice: The inclusion of the “Bagua,” concept of the figure 8 symbol, at the end of the session introduces a philosophical dimension, uniting physical movement with symbolic meaning. This connection elevates the practice beyond exercise, fostering a deeper sense of continuity, timelessness, and community among participants. It also implies that practice is not just a physical routine but a lifelong commitment to health and awareness.
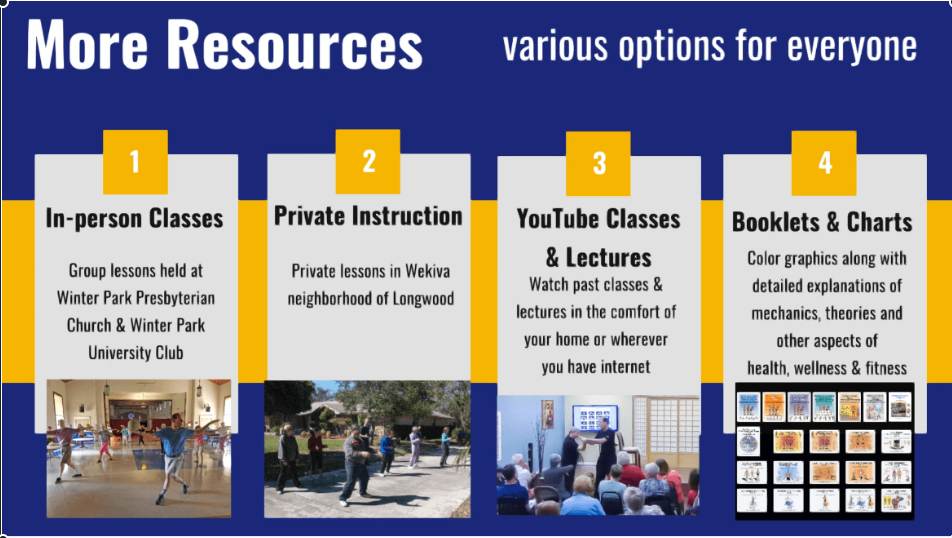
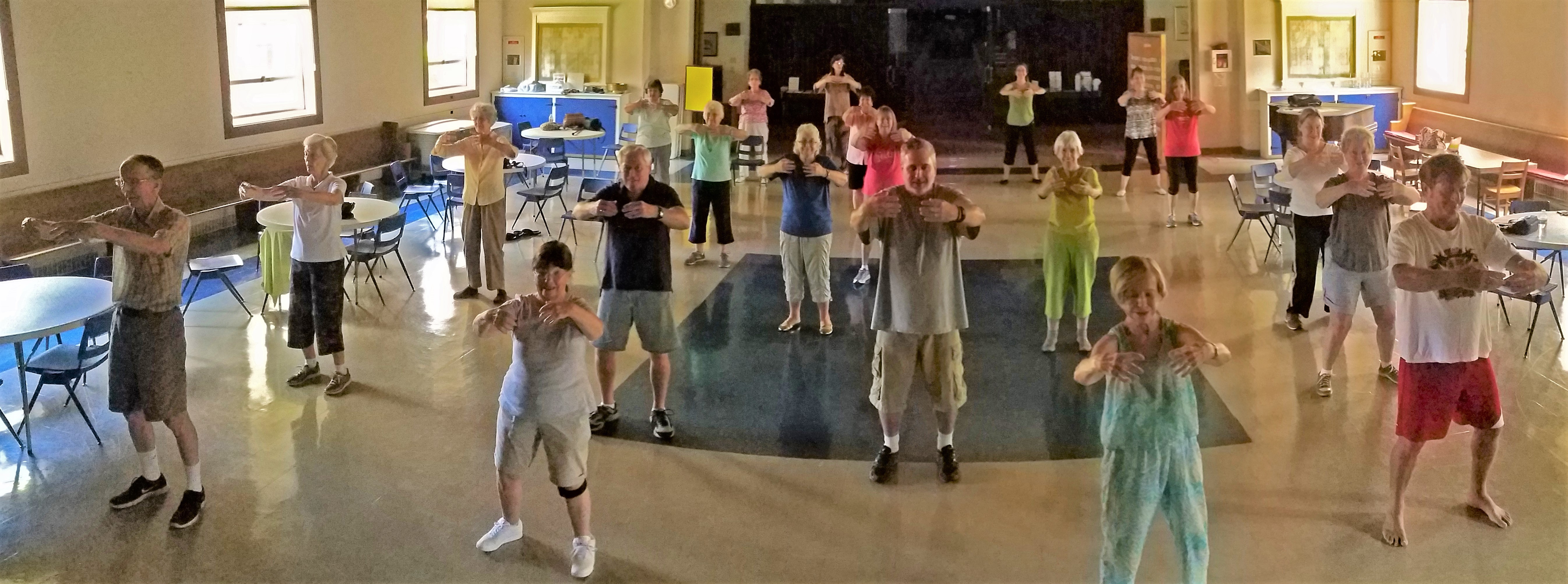
Longevity and Community Consistency Demonstrate Effectiveness: The fact that this class has been ongoing since 1997 illustrates the adaptability and effectiveness of these principles, as well as the strong community bonds formed among practitioners. The longevity also suggests that such practices can be sustainable and valuable throughout the decades, accommodating newcomers while preserving foundational wisdom. This longevity is a testament to the alignment of tradition with evolving modern health needs.
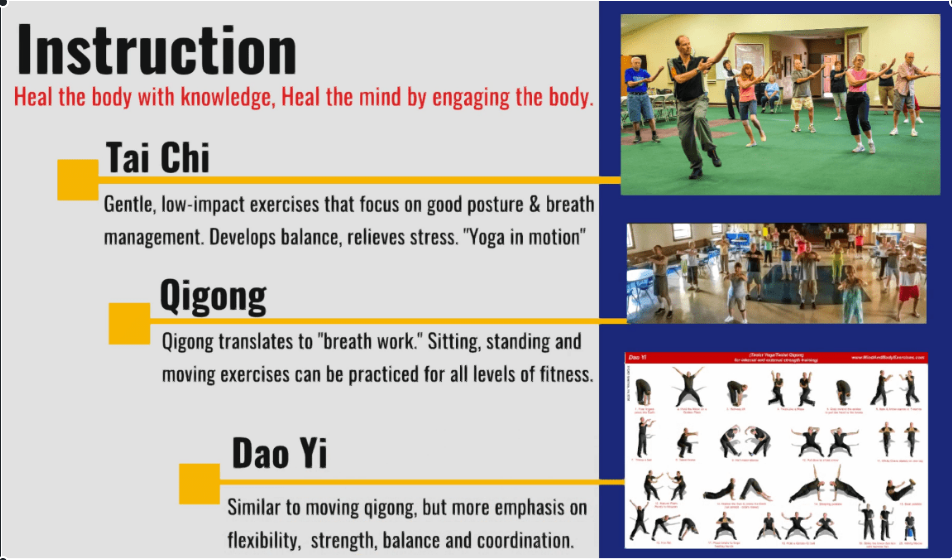
The video discusses a holistic approach to energy flow in the body, rooted in traditional Chinese medicine and similar philosophies. Unlike typical Western exercise which focuses primarily on cardiovascular activity and the heart, the practice highlighted here emphasizes the flow of energy through a sequence of organs and body parts, following natural patterns rather than symmetrical movements. This method promotes balanced and harmonious movement of energy and blood circulation throughout the body, providing greater overall health benefits.
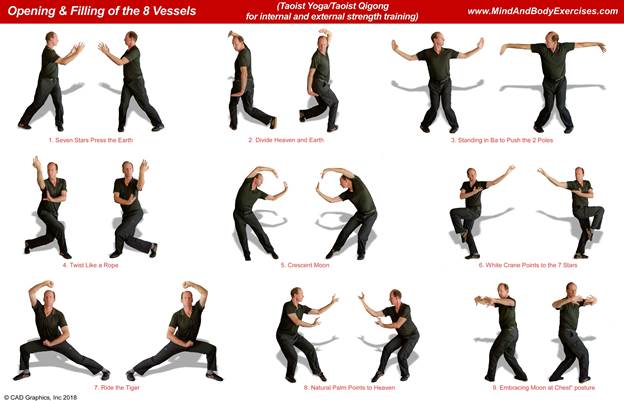
I guided participants through a closing set of movements designed to relax the major joints of the shoulders, elbows, wrists, hips, knees, ankles, while synchronizing breathing with mindful body awareness. This gradual cool-down process helps prevent muscle cramps and spasms common after mild or intense physical activity by gently bringing energy back to the body’s core “battery” or “bank account.” The collective movement and breath control encourage relaxation and prolonged breath holding through deliberate tension and release.
This holistic system blends ancient philosophy, breath work, energy theory, and joint mobility into one integrated practice. Rather than isolating fitness goals, it cultivates harmony between body and mind, reflecting the essence of Traditional Chinese Medicine: balanced energy, sustained vitality, and conscious movement.