Mount Kailash, located in the remote western region of the Tibetan Plateau, is not merely a geological marvel but a profound emblem of spiritual, mental, and physical integration. Revered across Hinduism, Buddhism, Jainism, and Bon, it stands as a living symbol of the interconnectedness that lies at the heart of holistic health. Rather than a site of conquest, it is a place of pilgrimage where the journey is inward, and the elevation sought is that of consciousness.
In Hindu philosophy, Mount Kailash is believed to be the dwelling place of Lord Shiva, the meditating ascetic who governs transformation and stillness. This vision mirrors a core tenet of holistic wellness, where there exists the need to cultivate inner awareness and transcendent consciousness. Shiva’s presence on the mountaintop symbolizes the crown chakra (sahasrara), representing union with the divine and the unfolding of higher consciousness (Johari, 2000).
Tibetan Buddhists identify the mountain as Kang Rinpoche, a manifestation of Mount Meru, or the cosmic axis believed to connect the heavens, earth, and underworld (Snellgrove, 1987). This symbolic vertical axis represents the human energetic spine in yogic practice and suggests that full alignment (both physical and spiritual) must occur from base to crown, a principle echoed in breathwork, qigong, and tai chi traditions.
In both spiritual and energetic models, Mount Kailash embodies balance and integration not only of body systems but of opposing forces: conscious and unconscious, effort and surrender, yin and yang.
The Kora: Pilgrimage as Mind-Body Practice
Pilgrims do not climb Mount Kailash. Instead, they perform a kora, which is a sacred circumambulation around the 52-kilometer base. This walking meditation reflects a form of dynamic mindfulness, an embodied spiritual practice that supports both mental clarity and physical endurance. It mirrors similar holistic practices such as walking meditation in Zen (Thich Nhat Hanh, 1991) and labyrinth walking in Western contemplative traditions.
One full kora is believed to absolve a lifetime of negative karma. Completing 108 cycles is said to lead to enlightenment. Regardless of belief system, this structured repetition and ritual movement demonstrate the psychophysiological benefits of contemplative physical exertion, a core aspect of holistic health (Bussing et al., 2012).
(Willaert, n.d.)
Psychosomatic Resonance and Symbolic Terrain
Mount Kailash’s position as the source of four major rivers (Indus, Sutlej, Brahmaputra, and Karnali) flowing in cardinal directions is symbolically rich. In traditional Chinese and Ayurvedic systems, water represents the flow of life force energy (qi or prana), and this geographical phenomenon reinforces Kailash’s status as a central energetic hub, a sacred “heart” of the world (Larre, de la Vallée, & Rochat de la Vallée, 1996).
The nearby lakes of Manasarovar (consciousness) and Rakshastal (unconscious or egoic forces) reflect archetypal and psychological dualities. Together, they offer a map of the inner self, where balance between light and shadow, awareness and instinct, becomes central to healing and integration (Jung, 1969).
Holistic Prohibition: Why Kailash Is Never Climbed
Unlike Everest, Kailash remains unclimbed by human feet, not due to physical danger but because of spiritual reverence. Ancient traditions prohibit accent, not as a denial of physical achievement, but as a call to humility, sacred restraint, and inner elevation. The modern holistic health movement increasingly acknowledges the power of respecting natural limits, recognizing that healing often arises not from forceful action but from honoring cycles, boundaries, and sacred stillness (Kabat-Zinn, 1990).
Myth, Energy, and Inner Ascent
Legends and esoteric traditions refer to Mount Kailash as a spiritual generator or vortex, a site of unexplained energetic phenomena. Though largely anecdotal, some studies of pilgrims’ experiences report states of heightened awareness, clarity, and emotional release, not unlike the effects of deep meditative states (Walach et al., 2005).
Holistically, Kailash becomes more than a destination. It is a mirror of the self, a metaphor for the inner path of transformation. The mountain teaches that healing, like the kora, requires movement around one’s core, integrating all aspects of being of mind, body, and spirit, until inner peace is restored.
Mount Kailash remains one of the Earth’s most revered sites, not because it has been conquered, but because it continues to conquer the ego. As a symbol of holistic integration, it reflects what modern wellness often seeks to rediscover: that true health is a sacred alignment, not just of body systems, but of the human spirit with the cosmos.
References:
Büssing, A., Michalsen, A., Khalsa, S. B. S., Telles, S., & Sherman, K. J. (2012). Effects of yoga on mental and physical health: A short summary of reviews. Evidence-Based Complementary and Alternative Medicine, 2012, 1–7. https://doi.org/10.1155/2012/165410
Jung, C. G. (1969). Collected Works of C.G. Jung, Volume 9 (Part 1): Archetypes and the Collective Unconscious (G. ADLER & R. F. C. HULL, Eds.). Princeton University Press. http://www.jstor.org/stable/j.ctt5hhrnk
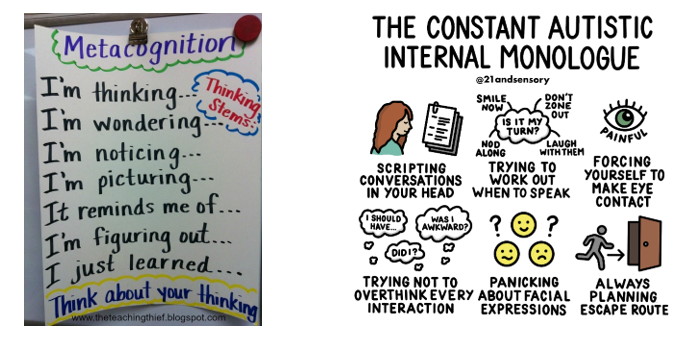
Holistic health emphasizes the integration of mind, body, and spirit. Within this framework, the ways in which we think about our thoughts and talk to ourselves internally play a central role in overall well-being. Two important but distinct psychological constructs, metacognition and the inner dialogue, form the foundation of self-awareness and self-regulation. While inner dialogue reflects the ongoing commentary of the mind, metacognition is the reflective process that evaluates and guides those thoughts. Understanding the distinction and interplay between the two provides powerful insight into mental, physical, and spiritual health.
Defining Metacognition
Metacognition, often described as “thinking about thinking,” refers to the awareness and regulation of one’s cognitive processes (Flavell, 1979). It includes both:
Metacognitive knowledge: recognizing one’s strengths, weaknesses, and strategies for thinking and learning.
Metacognitive regulation: the ability to plan, monitor, and adapt thought patterns and behaviors to reach goals (Schraw & Dennison, 1994).
For example, when someone recognizes they are struggling to focus and decides to change their study method or environment, they are applying metacognition. It functions as a higher-order system of self-observation, enabling intentional choices rather than automatic reactions.
Understanding the Inner Dialogue
The inner dialogue, also known as self-talk or inner speech, represents the continuous stream of words and judgments we silently direct toward ourselves. This internal commentary can be supportive (“I am capable of handling this challenge”) or critical (“I’ll never succeed at this”) (Morin, 2009). Unlike metacognition, which is strategic and reflective, inner dialogue is often spontaneous, shaped by prior experiences, beliefs, and emotional states (Beck, 2011).
Because inner dialogue can strongly influence emotion and physiology, triggering stress responses or enhancing motivation. It plays a direct role in daily wellness.
The Relationship Between Metacognition and Inner Dialogue
Although related, these two processes serve distinct roles:
Inner dialogue is the content of thought, with words, judgments, and narratives playing out in the mind.
Metacognition is the process that monitors and evaluates that content, determining whether it is useful, accurate, or aligned with one’s values and goals.
For example, a negative inner dialogue may say, “I am too tired to exercise.” Metacognition, however, can step in to evaluate this thought: “Is this fatigue physical exhaustion or just lack of motivation? What choice best supports my health goals?” This oversight allows individuals to reshape self-talk into a more adaptive pattern, such as: “I will start with a light walk to see how I feel.”
In this way, metacognition acts as a regulator of the inner dialogue, creating a feedback loop in which self-awareness leads to more balanced decisions.
Implications for Holistic Health and Wellness
Mental Wellness
Unchecked inner dialogue can amplify stress, worry, or self-doubt. Metacognition provides the awareness needed to identify unhelpful thought patterns, reduce rumination, and foster cognitive reappraisal (Wells, 2002). Metacognitive therapy, for example, helps individuals gain distance from destructive inner dialogue, improving resilience and emotional balance (Normann & Morina, 2018).
Physical Health
Health behaviors such as exercise, nutrition, and sleep are influenced by the interplay between self-talk and metacognition. Inner dialogue may discourage healthy action (“I don’t have time to cook tonight”), but metacognition allows for reflection and redirection (“If I prepare something simple now, I will feel better tomorrow”). Research suggests that higher levels of metacognitive awareness correlate with proactive health behaviors (Frazier et al., 2021).
Spiritual Growth
In the spiritual dimension of wellness, metacognition and inner dialogue intersect through practices such as meditation and prayer. Inner dialogue may be quieted, observed, or transformed during these practices, while metacognition supports discernment of which thoughts are distractions, and which carry deeper meaning (Vago & Silbersweig, 2012). This reflective process nurtures clarity, purpose, and transcendence—core elements of holistic health.
Practical Applications
Mindfulness and Meditation – Strengthen awareness of the inner dialogue and cultivate metacognitive observation without judgment.
Reflective Journaling – Encourage conscious monitoring of thought patterns, helping distinguish helpful from harmful self-talk.
Cognitive-Behavioral Practices – Use metacognition to challenge negative self-talk and reinforce positive, health-supporting narratives.
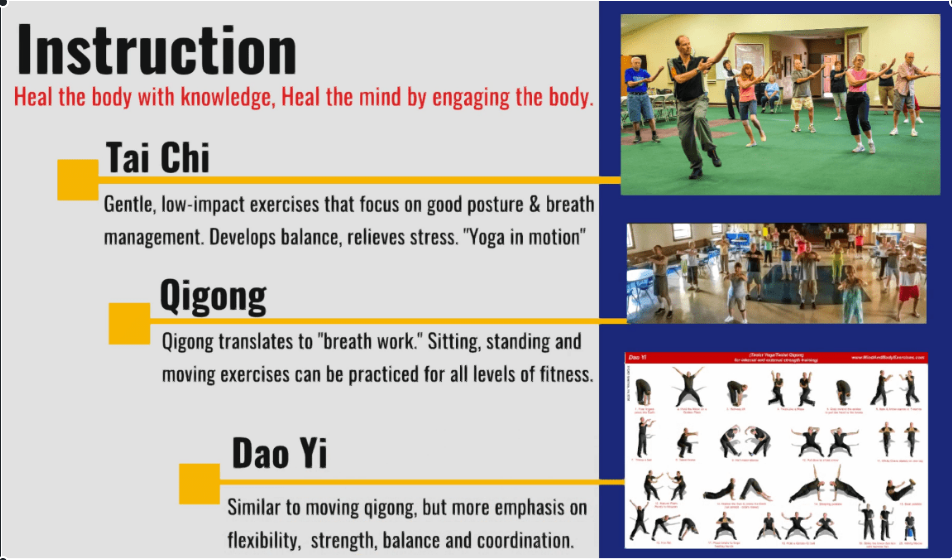
Holistic Disciplines (e.g., Tai Chi, Qigong, Yoga) – Integrate body awareness with reflective thought, aligning physical sensations with mindful inner regulation.
Metacognition and inner dialogue are distinct yet complementary processes that shape human experience. Inner dialogue provides the immediate content of thought, while metacognition serves as the higher-order process that monitors and reshapes those thoughts. Together, they influence mental clarity, physical choices, and spiritual insight, making them central to holistic health and wellness. By cultivating both awareness of the inner dialogue and the reflective power of metacognition, individuals can foster resilience, self-regulation, and a deeper sense of integration across mind, body, and spirit.
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive–developmental inquiry. American Psychologist, 34(10), 906–911. https://doi.org/10.1037/0003-066x.34.10.906
Frazier, L. D., Schwartz, B. L., & Metcalfe, J. (2021). The MAPS model of self-regulation: Integrating metacognition, agency, and possible selves. Metacognition and Learning, 16(2), 297–318. https://doi.org/10.1007/s11409-020-09255-3
Morin, A. (2009). Self-awareness deficits following loss of inner speech: Dr. Jill Bolte Taylor’s case study. Consciousness and Cognition, 18(2), 524–529. https://doi.org/10.1016/j.concog.2008.09.008
Normann, N., & Morina, N. (2018). The efficacy of metacognitive therapy: A systematic review and meta-analysis. Frontiers in Psychology, 9, 2211. https://doi.org/10.3389/fpsyg.2018.02211
Schraw, G., & Dennison, R. S. (1994). Assessing metacognitive awareness. Contemporary Educational Psychology, 19(4), 460–475. https://doi.org/10.1006/ceps.1994.1033
Vago, D. R., & Silbersweig, D. A. (2012). Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Frontiers in Human Neuroscience, 6, 296. https://doi.org/10.3389/fnhum.2012.00296
Winter, Immunity, and the Unsustainable Model of Modern Healthcare. Why Lifestyle Medicine Must Become the First Line of Defense
Winter has long been recognized as a season of heightened illness, commonly referred to as “flu season.” This pattern has existed for thousands of years, shaped by environmental conditions, reduced sunlight, behavioral changes, and altered activity patterns. Yet despite humanity’s long-standing awareness of these seasonal rhythms, modern healthcare systems, particularly in the United States, continue to respond with a predominantly pharmaceutical-centered model. Vaccines and medications are promoted as the primary line of defense, while foundational health behaviors such as nutrition, movement, sunlight exposure, sleep, and stress regulation receive comparatively little emphasis.
You can watch my short video on this topic at:
This strategy is proving unsustainable. The United States now faces a continuous decline in both physical and mental health, rising chronic disease burden, escalating healthcare costs, and worsening quality of life indicators. The growing reliance on pharmaceutical intervention without addressing underlying behavioral and environmental contributors has created a reactive, symptom-focused system rather than a proactive, resilience-based model of health. This essay argues that a fundamental reorientation toward lifestyle medicine as the primary foundation of public health is not only logical, but essential for reversing current health trajectories.
The Predictable Nature of Winter Illness
Seasonal illness is not random. Respiratory infections, influenza, and other viral illnesses consistently peak during winter months due to a convergence of physiological, behavioral, and environmental factors. These include increased indoor crowding, reduced physical activity, poorer dietary habits, higher alcohol consumption, disrupted sleep, and reduced exposure to sunlight (Eccles, 2002; Dowell & Ho, 2004).
Human physiology evolved in close relationship with seasonal rhythms. Historically, winter was a period of reduced food availability, lower caloric intake, and continued physical labor. In contrast, modern winter behavior is characterized by caloric excess, sedentary lifestyles, and prolonged indoor confinement, conditions that directly suppress immune function and metabolic health (Booth et al., 2012).
The seasonal rise in illness is therefore not an unavoidable biological fate, but a predictable consequence of modern lifestyle patterns layered onto ancient physiology.
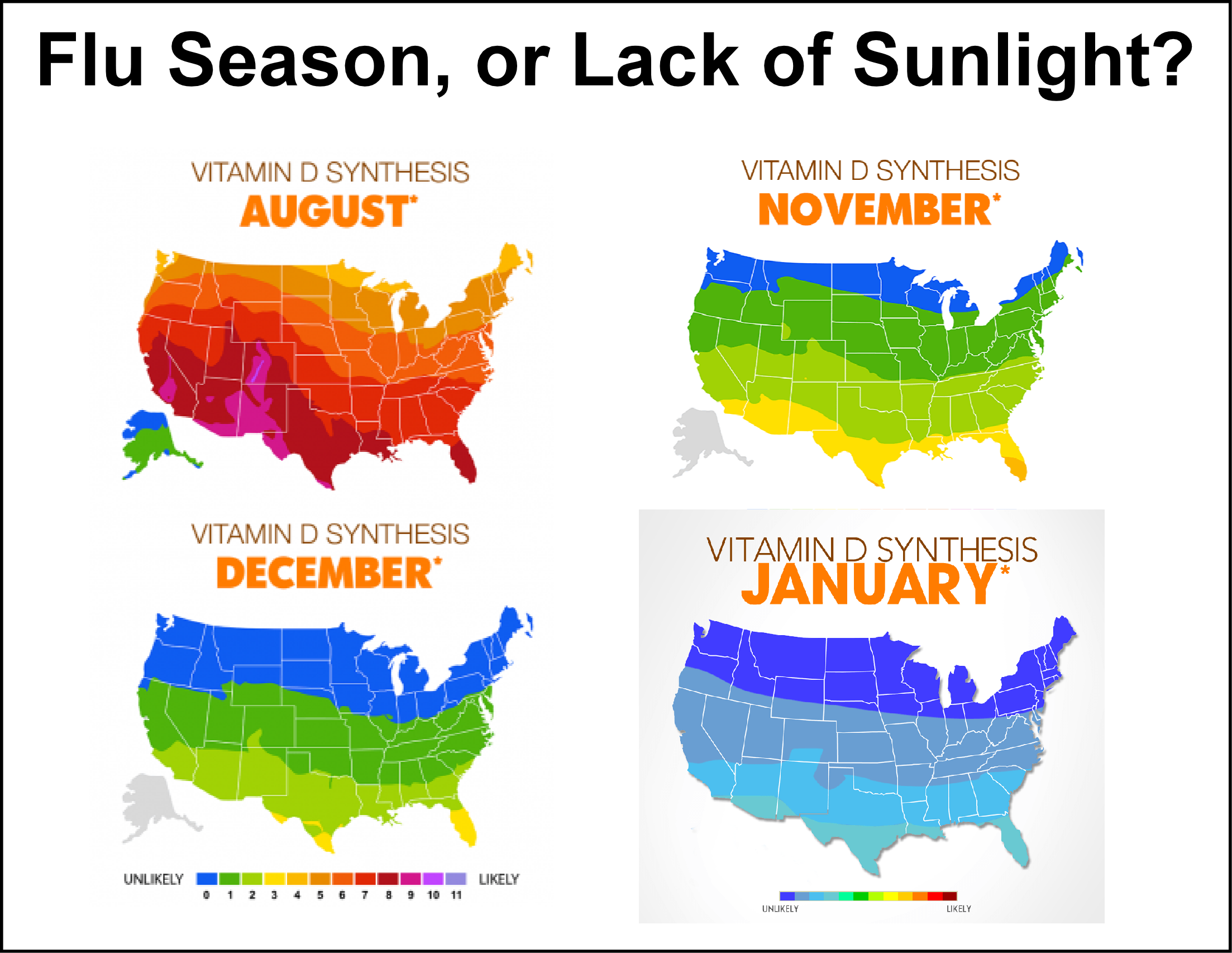
Vitamin D Deficiency: A Global and Seasonal Crisis
One of the most significant contributors to winter immune vulnerability is widespread vitamin D deficiency. Vitamin D synthesis is dependent on ultraviolet B (UVB) radiation from sunlight, which is largely absent during winter months in northern latitudes. As a result, deficiency rates increase dramatically during this season.
Globally, over one billion people are estimated to be vitamin D deficient (Holick, 2007). In the United States, approximately 40–60% of adults have insufficient levels during winter months (Forrest & Stuhldreher, 2011). Vitamin D plays a central role in immune regulation, influencing innate immunity, T-cell function, and inflammatory control (Aranow, 2011).
Low vitamin D levels are associated with increased risk of respiratory infections, influenza, autoimmune disease, and poorer outcomes in viral illness (Martineau et al., 2017; Gombart et al., 2020). Yet despite this robust evidence base, vitamin D status is rarely assessed or addressed in routine clinical care.
Physical Inactivity and Immune Suppression
Physical activity is one of the most powerful modulators of immune function. Regular movement enhances immune surveillance, improves lymphatic circulation, reduces chronic inflammation, and improves metabolic health (Nieman & Wentz, 2019).
Conversely, physical inactivity, now widespread in industrialized nations, has been shown to increase susceptibility to infection, worsen vaccine response, and promote chronic low-grade inflammation (Booth et al., 2012; Hamer et al., 2020). Winter months exacerbate sedentary behavior, as colder temperatures and shorter daylight hours reduce outdoor activity.
The modern human body, designed for daily movement, now spends most of its time in chairs, cars, and climate-controlled environments. This mismatch between evolutionary design and modern behavior contributes directly to immune dysfunction and chronic disease.
Ultra-Processed Food and Immune Dysfunction
Diet quality is another central determinant of immune health. Modern winter diets are often dominated by ultra-processed foods high in refined carbohydrates, industrial seed oils, additives, preservatives, and sugar. These foods disrupt gut microbiota, promote insulin resistance, increase systemic inflammation, and impair immune signaling (Monteiro et al., 2018; Zinöcker & Lindseth, 2018).
The gut microbiome plays a critical role in immune regulation, with approximately 70% of immune cells residing in gut-associated lymphoid tissue (Belkaid & Hand, 2014). Diets rich in whole foods, vegetables, fruits, legumes, lean proteins, and healthy fats, support microbial diversity and immune resilience, while ultra-processed foods degrade this vital ecosystem.
The widespread replacement of traditional diets with industrial food products represents one of the most profound biological experiments in human history, and its results are increasingly evident in rising rates of obesity, diabetes, autoimmune disease, depression, and cardiovascular illness.
Mental Health Decline and Immune Consequences
The decline in mental health over recent decades parallels the deterioration of physical health. Rates of anxiety, depression, substance abuse, and suicide have risen sharply in the United States (Twenge et al., 2019; CDC, 2023). Chronic psychological stress suppresses immune function through dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis and increased cortisol exposure (Glaser & Kiecolt-Glaser, 2005).
Social isolation, now increasingly common further compounds this effect. Loneliness has been shown to increase inflammatory signaling and reduce antiviral immune responses (Hawkley & Cacioppo, 2010). Winter confinement and digital substitution for human connection intensify this problem.
The modern epidemic of loneliness, combined with chronic stress and digital overexposure, represents a silent immune suppressant operating year-round.
The Reactive Model of Modern Healthcare
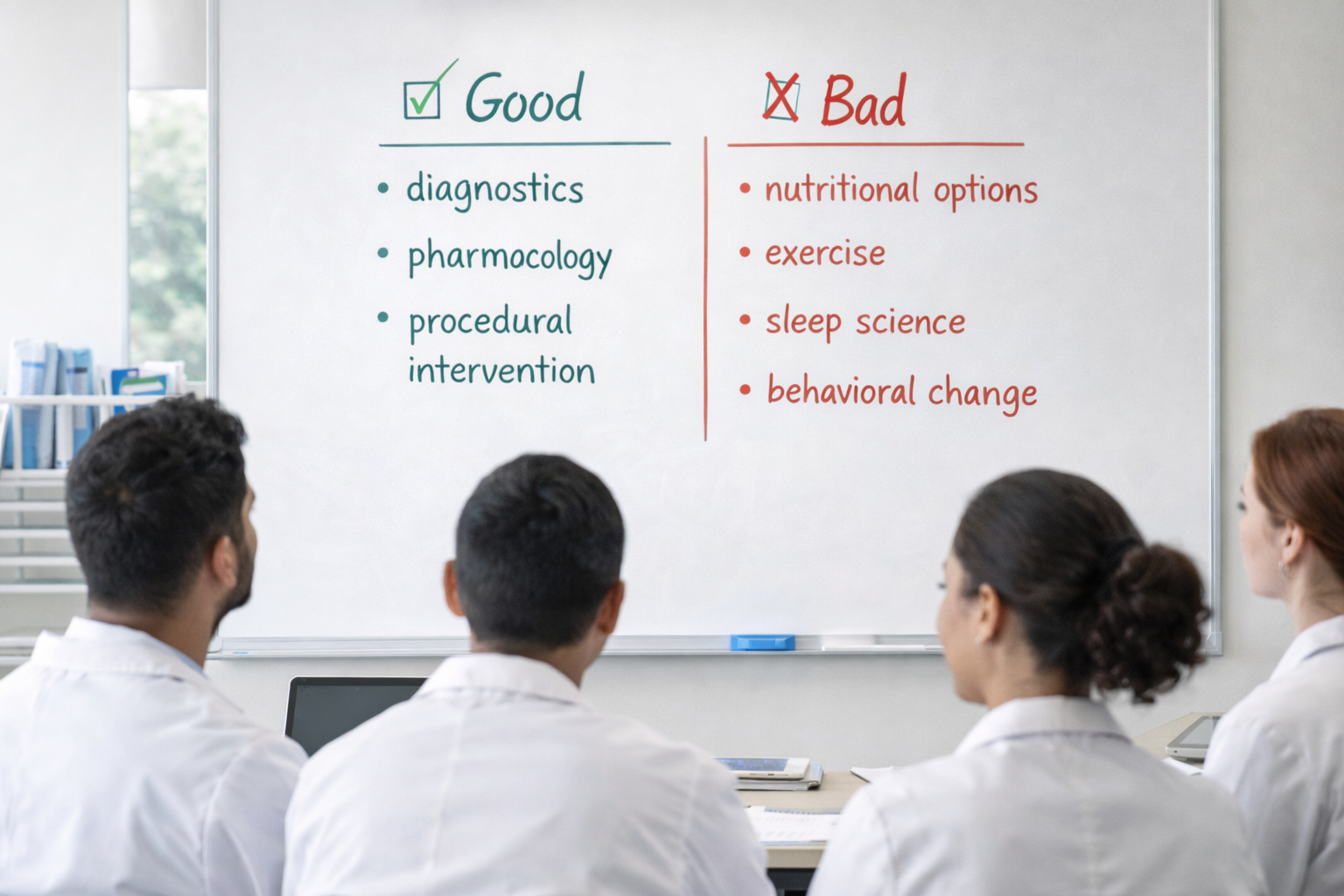
The current healthcare system in the United States is primarily structured around disease management rather than health creation. Physicians receive minimal training in nutrition, exercise physiology, sleep science, or behavioral change counseling (Adams et al., 2010; Devries et al., 2019). As a result, clinical encounters are dominated by diagnostics, pharmacology, and procedural intervention.
This model is highly effective for acute trauma and infectious disease management. However, it is poorly suited for addressing chronic, lifestyle-driven illnesses. The system is financially incentivized to treat disease after it develops rather than prevent it from occurring.
Vaccines and medications are promoted as population-level solutions because they can be standardized, deployed rapidly, and measured easily. Lifestyle change, by contrast, requires time, education, accountability, and cultural transformation.
The result is a healthcare system that waits for illness to emerge rather than building resilient physiology in advance.
The Unsustainable Trajectory of U.S. Health
Despite spending more on healthcare than any nation in the world, the United States ranks poorly in life expectancy, chronic disease burden, and quality-of-life metrics (Tikkanen & Abrams, 2020). Obesity rates exceed 40%, diabetes affects over 11% of adults, and cardiovascular disease remains the leading cause of death (CDC, 2023).
Mental health outcomes have deteriorated alongside physical health. The pharmaceutical expansion has not reversed these trends. Instead, the nation now consumes more prescription medications per capita than any other country while continuing to grow sicker.
This trajectory is not sustainable economically, biologically, or socially.
Reclaiming the Logical Hierarchy of Health
Human physiology evolved in an environment defined by:
Daily physical labor
Seasonal sunlight exposure
Whole-food nutrition
Natural circadian rhythms
Social cooperation
Environmental challenge
Modern life has inverted these conditions. The logical hierarchy of health must be restored:
Nutrition quality
Physical movement
Sleep hygiene
Sunlight exposure
Stress regulation
Social connection
Medical intervention when necessary
Pharmaceuticals should function as supportive tools—not the foundation of human health.
This integrative model does not reject medicine. It restores medicine to its proper role.
Winter illness is not merely a seasonal inconvenience, it is a symptom of a broader systemic failure to align modern life with human biology. The current healthcare model, built on pharmaceutical intervention rather than physiological resilience, is incapable of reversing the ongoing decline in physical and mental health.
Encouraging better nutrition, more movement, adequate sunlight exposure, sufficient sleep, stress regulation, and social connection is not alternative medicine. It is foundational medicine.
Without a return to these biological essentials, no number of pharmaceuticals will reverse the trajectory of modern disease. The future of healthcare must shift from managing illness to cultivating health. Only then can winter become a season of resilience rather than vulnerability.
References:
Adams, K. M., Kohlmeier, M., Powell, M., & Zeisel, S. H. (2010). Nutrition in medicine: nutrition education for medical students and residents. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition, 25(5), 471–480. https://doi.org/10.1177/0884533610379606
Booth, F. W., Roberts, C. K., & Laye, M. J. (2012). Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology, 2(2), 1143–1211. https://doi.org/10.1002/cphy.c110025
Centers for Disease Control and Prevention. (2023). Chronic disease indicators and mental health statistics. https://www.cdc.gov
Devries, S., Dalen, J. E., Eisenberg, D. M., Maizes, V., Ornish, D., Prasad, A., Sierpina, V., Weil, A. T., & Willett, W. (2014). A deficiency of nutrition education in medical training. The American journal of medicine, 127(9), 804–806. https://doi.org/10.1016/j.amjmed.2014.04.003
Dowell, S. F., & Ho, M. S. (2004). Seasonality of infectious diseases and severe acute respiratory syndrome—What we don’t know can hurt us. The Lancet Infectious Diseases, 4(11), 704–708. https://doi.org/10.1016/S1473-3099(04)01177-6
Eccles, R. (2002). An explanation for the seasonality of acute upper respiratory tract viral infections. Acta Oto-Laryngologica, 122(2), 183–191. https://doi.org/10.1080/00016480252814207
Forrest, K. Y. Z., & Stuhldreher, W. L. (2011). Prevalence and correlates of vitamin D deficiency in US adults. Nutrition Research, 31(1), 48–54. https://doi.org/10.1016/j.nutres.2010.12.001
Glaser, R., & Kiecolt-Glaser, J. K. (2005). Stress-induced immune dysfunction. Nature Reviews Immunology, 5(3), 243–251. https://doi.org/10.1038/nri1571
Gombart, A. F., Pierre, A., & Maggini, S. (2020). A review of micronutrients and the immune system. Nutrients, 12(1), 236. https://doi.org/10.3390/nu12010236
Hamer, M., Kivimäki, M., Gale, C. R., & Batty, G. D. (2020). Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain, behavior, and immunity, 87, 184–187. https://doi.org/10.1016/j.bbi.2020.05.059
Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Annals of behavioral medicine : a publication of the Society of Behavioral Medicine, 40(2), 218–227. https://doi.org/10.1007/s12160-010-9210-8
Martineau, A. R., et al. (2017). Vitamin D supplementation to prevent acute respiratory tract infections. BMJ, 356, i6583. https://doi.org/10.1136/bmj.i6583
Monteiro, C. A., Cannon, G., Moubarac, J. C., Levy, R. B., Louzada, M. L. C., & Jaime, P. C. (2018, January 1). The un Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutrition. Cambridge University Press. https://doi.org/10.1017/S1368980017000234
Nieman, D. C., & Wentz, L. M. (2019). The compelling link between physical activity and the body’s defense system. Journal of sport and health science, 8(3), 201–217. https://doi.org/10.1016/j.jshs.2018.09.009
Twenge, J. M., Cooper, A. B., Joiner, T. E., Duffy, M. E., & Binau, S. G. (2019). Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005-2017. Journal of abnormal psychology, 128(3), 185–199. https://doi.org/10.1037/abn0000410
Zinöcker, M. K., & Lindseth, I. A. (2018). The Western Diet-Microbiome-Host Interaction and Its Role in Metabolic Disease. Nutrients, 10(3), 365. https://doi.org/10.3390/nu10030365
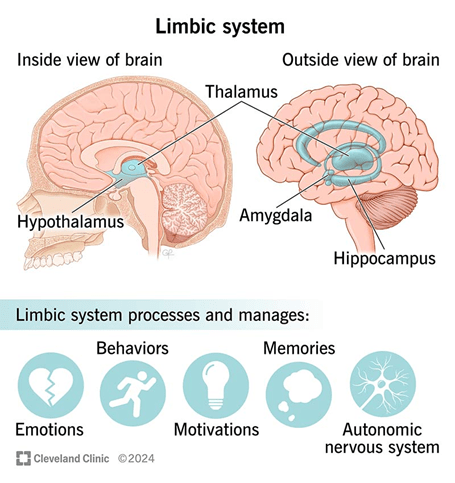
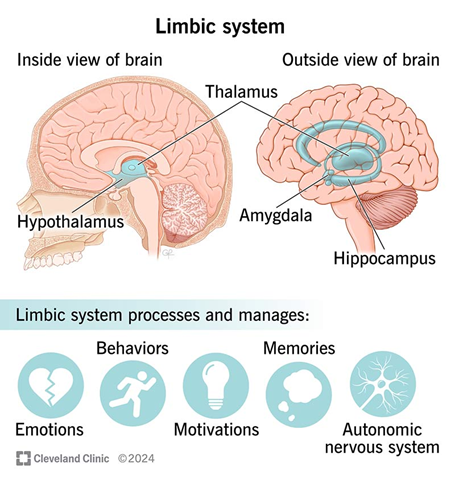
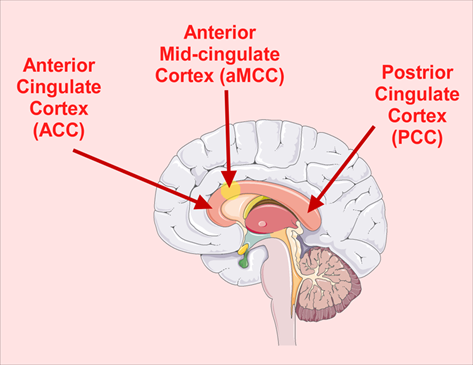
Pain is not solely a sensory experience. It is also deeply emotional, influenced by context, memory, expectation, and mood. While the somatosensory cortex processes the discriminative (sensory) aspects of pain, such as location, intensity, and duration, the limbic system, particularly the amygdala and the anterior cingulate cortex (ACC), mediates its affective (emotional) and motivational components (Apkarian et al., 2005; Leknes & Tracey, 2008).
1. The Amygdala: Fear, Salience, and Emotional Memory
The amygdala is a central structure in emotional processing, especially in the encoding and recall of fear and threat-related memories. It plays a critical role in the emotional coloring of pain and how we anticipate and respond to it.
The amygdala receives nociceptive input via the spino-parabrachial pathway and from higher-order cortical areas, allowing it to influence both immediate emotional reactions to pain and pain-related memory (Neugebauer et al., 2004).
It activates autonomic and behavioral responses to pain (e.g., anxiety, avoidance), especially when pain is perceived as threatening or unpredictable.
Amygdala hyperactivity has been linked with chronic pain conditions, where emotional reactivity and threat perception become amplified (Simons et al., 2014).
In other words, the amygdala adds emotional salience to nociceptive stimuli, transforming a mere sensory signal into a subjectively distressing experience.
2. The Anterior Cingulate Cortex (ACC): The Distress and Motivation Circuit
The ACC, particularly its rostral and dorsal regions, plays a central role in pain unpleasantness, emotional suffering, and motivational drive to escape or alleviate pain.
Studies show that ACC activation correlates with subjective pain unpleasantness, even when the physical intensity of pain is constant (Rainville et al., 1997).
The ACC is richly interconnected with limbic (amygdala, hippocampus), cognitive (prefrontal cortex), and motor systems, enabling it to integrate affective, attentional, and behavioral responses to pain (Shackman et al., 2011).
The ACC is involved in pain anticipation, which can amplify emotional distress even before the pain occurs (Koyama et al., 2005).
Chronic pain patients often show structural and functional changes in the ACC, suggesting a maladaptive feedback loop that reinforces pain-related suffering (Baliki et al., 2006).
Thus, the ACC is not responsible for detecting pain, but for how unpleasant and distressing it feels, and for driving the motivational state to take action.
3. Limbic Modulation and Homeostasis
Leknes & Tracey (2008) propose a framework for understanding how pain and pleasure share overlapping neurobiological systems, particularly in limbic circuits. They note that context, expectation, and emotional state can either amplify or dampen pain via top-down modulation of limbic and brainstem structures.
The ACC and amygdala are sensitive to emotional reappraisal, social support, and placebo analgesia, demonstrating that the emotional meaning of pain can drastically change the experience (Wager et al., 2004).
Pain that is interpreted as meaningful or self-chosen (e.g., in rituals or athletic endurance) can be experienced as less unpleasant, implicating limbic regulation of pain perception (Leknes & Tracey, 2008).
This suggests that the limbic system is central in determining whether pain is perceived as threatening and intolerable or manageable and meaningful.
4. Summary of Functional Roles
Region
Role in Pain Processing
Amygdala
Assigns emotional salience; fear, anxiety, memory of pain; enhances pain when perceived as threatening.
ACC
Encodes pain unpleasantness; mediates suffering, motivation to escape pain; modulated by expectation, attention, and emotional context.
Clinical Relevance
Chronic pain syndromes (e.g., fibromyalgia, neuropathic pain) often involve heightened activity in the amygdala and ACC, contributing to emotional suffering, catastrophizing, and avoidance behavior (Hashmi et al., 2013).
Cognitive-behavioral therapy (CBT), mindfulness, and biofeedback target these limbic circuits to reframe pain perception, reduce suffering, and restore functional coping.
The limbic-emotional dimension of pain underscores the importance of holistic and biopsychosocial models in treatment.
References:
Apkarian, A. V., Bushnell, M. C., Treede, R. D., & Zubieta, J. K. (2005). Human brain mechanisms of pain perception and regulation in health and disease. European Journal of Pain, 9(4), 463–484. https://doi.org/10.1016/j.ejpain.2004.11.001
Baliki, M. N., Geha, P. Y., Apkarian, A. V., & Chialvo, D. R. (2006). Beyond feeling: chronic pain hurts the brain, disrupting the default-mode network dynamics. Journal of Neuroscience, 28(6), 1398–1403. https://doi.org/10.1523/JNEUROSCI.4123-07.2008
Hashmi, J. A., Baliki, M. N., Huang, L., Baria, A. T., Torbey, S., Hermann, K. M., … & Apkarian, A. V. (2013). Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain, 136(9), 2751–2768. https://doi.org/10.1093/brain/awt211
Koyama, T., McHaffie, J. G., Laurienti, P. J., & Coghill, R. C. (2005). The subjective experience of pain: Where expectations become reality. Proceedings of the National Academy of Sciences of the United States of America, 102(36), 12950–12955. https://doi.org/10.1073/pnas.0408576102
Leknes, S., & Tracey, I. (2008). A common neurobiology for pain and pleasure. Nature Reviews Neuroscience, 9(4), 314–320. https://doi.org/10.1038/nrn2333
Rainville, P., Duncan, G. H., Price, D. D., Carrier, B., & Bushnell, M. C. (1997). Pain affect encoded in human anterior cingulate but not somatosensory cortex. Science, 277(5328), 968–971. https://doi.org/10.1126/science.277.5328.968
Shackman, A. J., Salomons, T. V., Slagter, H. A., Fox, A. S., Winter, J. J., & Davidson, R. J. (2011). The integration of negative affect, pain and cognitive control in the cingulate cortex. Nature Reviews Neuroscience, 12(3), 154–167. https://doi.org/10.1038/nrn2994
Simons, L. E., Elman, I., & Borsook, D. (2014). Psychological processing in chronic pain: a neural systems approach. Neuroscience & Biobehavioral Reviews, 39, 61–78. https://doi.org/10.1016/j.neubiorev.2013.12.006
Wager, T. D., Rilling, J. K., Smith, E. E., Sokolik, A., Casey, K. L., Davidson, R. J., … & Cohen, J. D. (2004). Placebo-induced changes in FMRI in the anticipation and experience of pain. Science, 303(5661), 1162–1167. https://doi.org/10.1126/science.1093065
Trauma rarely arrives by invitation. For most people, it enters life unexpectedly, through loss, betrayal, illness, accidents, violence, neglect, coercion, or prolonged stress. Very few individuals seek out traumatic experiences, and just as rarely do most people consciously intend to harm or traumatize others. And yet, despite intent, all actions carry consequences. Words spoken in anger, choices made in fear, systems built on imbalance, and moments of inattention can send ripple effects outward for years, sometimes for generations. Trauma often lives in these ripples.
Long after the original event has passed, many people continue to feel unsettled inside, anxious, guarded, emotionally numb, reactive, ashamed, or unsure of who they have become. These experiences are not signs of weakness or personal failure. They are the natural imprint of overwhelming stress on the nervous system, identity, and relational trust. Trauma changes how the body responds to threat, how the mind interprets reality, how the self is organized, and how relationships are navigated.
My book Post-traumatic Growth – Essays to Cultivate Healing, Integration, and Meaning was written for those who have survived difficult experiences and now find themselves asking deeper questions, not only how to cope, but how to truly grow beyond survival. The gradual cultivation of healing and growth does not mean that trauma was good, necessary, deserved, or spiritually justified. It does not minimize suffering or attempt to frame pain as a gift. Rather, it acknowledges a well-documented truth: human beings possess a powerful capacity to adapt, integrate, mature, and rebuild their lives when safety, awareness, and agency are gradually restored.
For decades, my work has focused on the relationship between stress physiology, emotional regulation, behavior, identity, and resilience. Again and again, I have seen that trauma recovery is not only psychological. It is neurological. It is relational. It is embodied. Insight alone is not enough. Healing requires the reorganization of the nervous system, the development of emotional maturity, the rebuilding of boundaries, the restoration of agency, and the reconstruction of meaning.
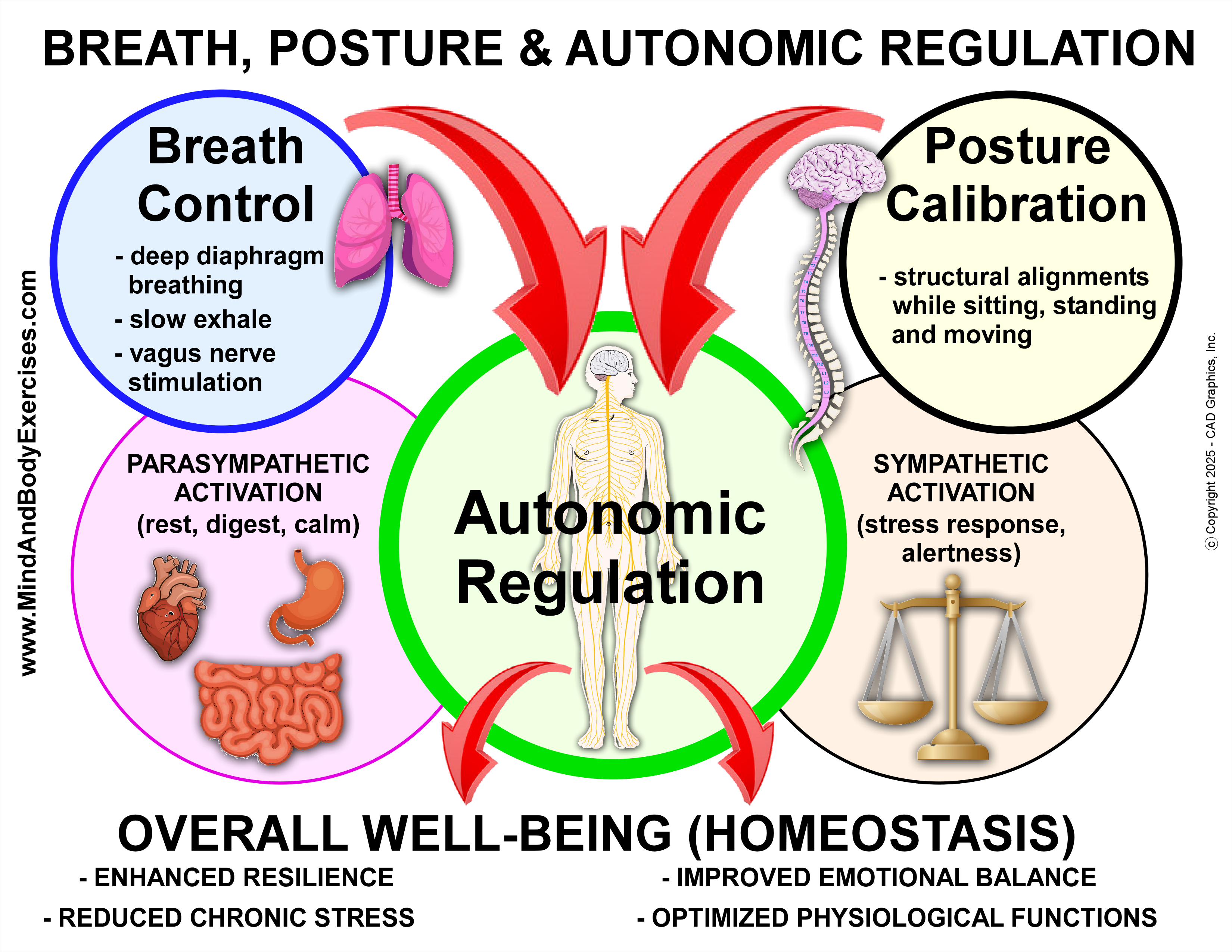
This book follows the full arc of transformation. It begins with how trauma disrupts regulation, perception, and identity. It then moves into the practical foundations of recovery by using breath, posture, emotional regulation, and stress resilience. From there, it addresses the deeper psychological work of boundaries, meaning-making, emotional maturity, and agency. Finally, it turns outward toward contribution, service, and the lifelong process of integration and wholeness.
If you are reading this, it is likely because some part of your life has been shaped by adversity, sudden or prolonged, visible or hidden. This book does not offer shortcuts. It offers something more enduring: a grounded path toward rebuilding stability, identity, agency, and meaning over time. These essays are not meant to be rushed or consumed linearly, but revisited as one’s capacity for regulation, reflection, and integration deepens. Growth does not erase the past. It allows you to live no longer defined by it.


















{kind=link}